Miễn phí
Hẹp hạ thanh môn mắc phải ở trẻ nhũ nhi 2 tháng tuổi sau khi đặt nội khí quản kéo dài liên quan đến viêm phổi do ho gà: Một báo cáo ca bệnh
Acquired Subglottic Stenosis in a 2-Month-Old Infant After Prolonged Intubation Associated With Pertussis Pneumonia: A Case Report
Yun-Gai Cheng; Xiao-Fen Tao; Xu Dan; Xue-Jing Li; Lei Wu; Xi-Ling Wu. American Journal of Case Reports. doi: 10.12659/AJCR.948709. Open access.
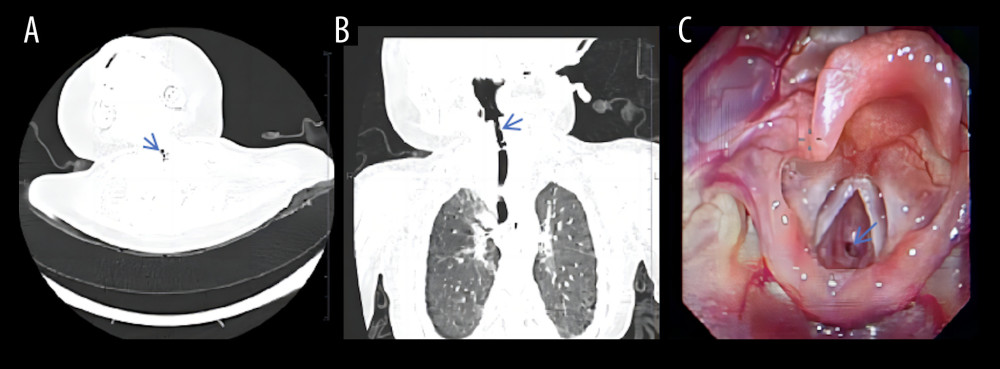
Figure 1
https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e948709-g001.jpg&idArt=948709&w=1000
Figure 1
Hình 1
Neck and chest computed tomography scans (A, B) demonstrated localized subglottic stenosis. Fiber laryngoscopy (C) revealed severe subglottic stenosis with a pinhole-sized lumen.
Chụp cắt lớp vi tính vùng cổ và ngực (A, B) cho thấy tình trạng hẹp hạ thanh môn khu trú. Nội soi thanh quản ống mềm (C) cho thấy hẹp hạ thanh môn nghiêm trọng với lòng đường thở chỉ còn kích thước bằng đầu kim.
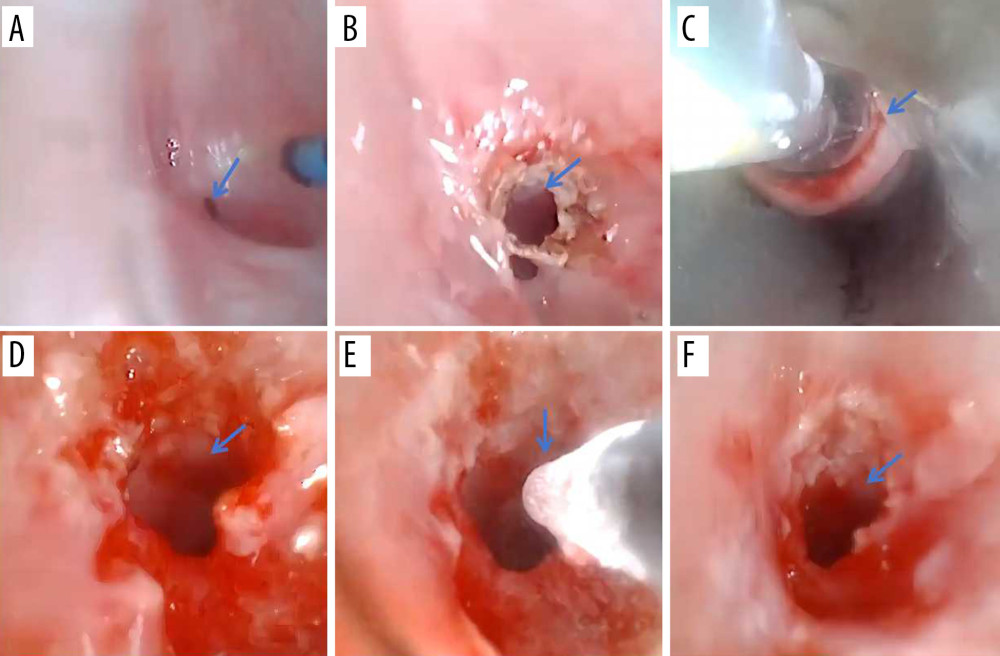
Figure 2
https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e948709-g002.jpg&idArt=948709&w=1000
Figure 2
Hình 2
Bronchoscopic interventional treatment of subglottic stenosis and postoperative airway. (A) Bronchoscopy before therapy revealed airway stenosis. (B–E) Holmium laser, balloon dilation, and cryotherapy were performed to treat the stenotic region. (F) After the first intervention, the airway lumen was considerably enlarged.
Điều trị can thiệp qua nội soi phế quản đối với hẹp hạ thanh môn và đường thở sau phẫu thuật. (A) Nội soi phế quản trước khi điều trị cho thấy tình trạng hẹp đường thở. (B–E) Laser holmium, nong bóng và liệu pháp áp lạnh đã được thực hiện để điều trị vùng bị hẹp. (F) Sau can thiệp lần đầu, lòng đường thở đã được mở rộng đáng kể.
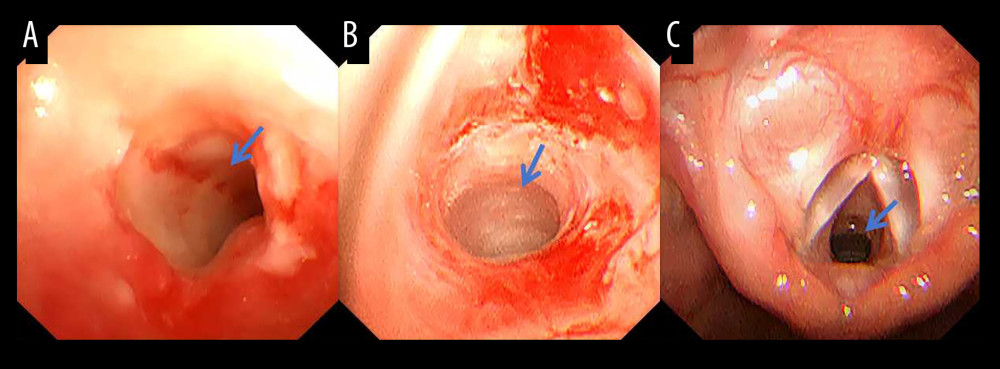
Figure 3
https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e948709-g003.jpg&idArt=948709&w=1000
Figure 3
Hình 3
(A) Bronchoscopy on postoperative day 4 and (B) 2 weeks later revealed clinically significant improvement in airway patency. (C) One month postoperatively, fiber laryngoscopy showed complete resolution of stenosis
(A) Nội soi phế quản vào ngày thứ 4 sau phẫu thuật và (B) 2 tuần sau đó cho thấy sự cải thiện đáng kể về mặt lâm sàng đối với độ thông thoáng đường thở. (C) Một tháng sau phẫu thuật, nội soi thanh quản ống mềm cho thấy tình trạng hẹp đã được giải quyết hoàn toàn.
Có thể bạn quan tâm
-
Giảm tiểu cầu liên quan đến ethambutol: Báo cáo ca lâm sàng hiếm gặp về tình trạng giảm tiểu cầu do thuốc trong điều trị lao
Ethambutol-Associated Thrombocytopenia: A Rare Case Report of Drug-Induced Platelet Decline in Tuberculosis Treatment
-
Tập luyện ngắt quãng cường độ cao nhằm giảm hội chứng chuyển hóa tim mạch ở nhóm dân số khỏe mạnh nhưng ít vận động
High-intensity interval training for reducing cardiometabolic syndrome in healthy but sedentary populations
-
Có an toàn khi sử dụng bột và phẩm màu trang trí bánh không? 2 chuyên gia giải thích
Is it safe to use cake decorating dusts and dyes? 2 experts explain