Ca lâm sàng
Hội chứng Guillain-Barré trong tam cá nguyệt thứ ba của thai kỳ: Báo cáo ca bệnh và tổng quan y văn
Guillain-Barré Syndrome in the Third Trimester of Pregnancy: A Case Report and Literature Review
Liang Gao; Mouchang Qiu; Hua Qian. American Journal of Case Reports. doi: 10.12659/AJCR.949852. Open access.
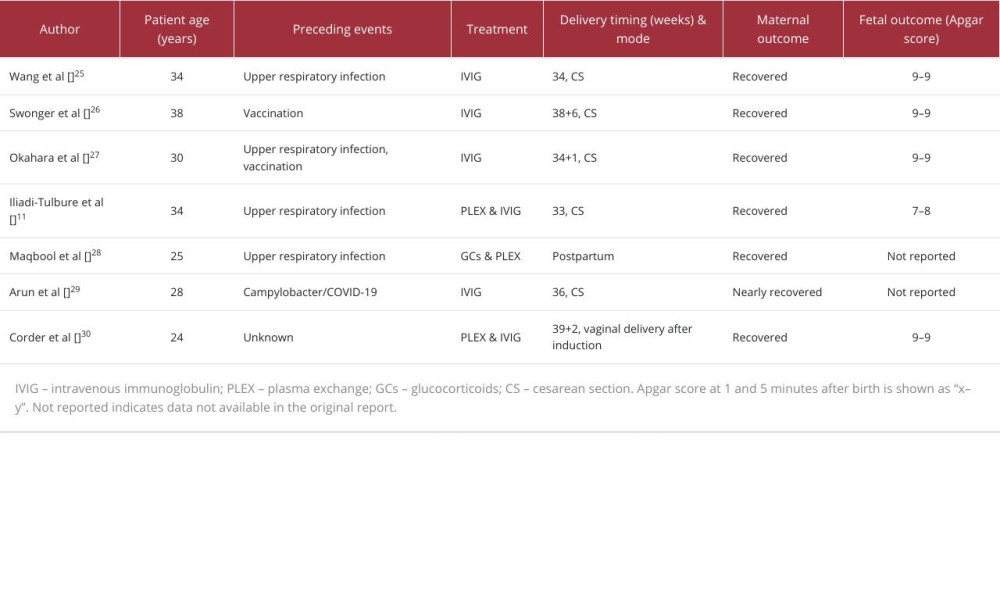
Table 1
https://jours.isi-science.com/imageXml.php?i=t1-amjcaserep-26-e949852.jpg&idArt=949852&w=1000
Table 1
Bảng 1
Summary of reported cases of Guillain-Barré syndrome (GBS) during pregnancy and postpartum.
Tóm tắt các ca bệnh hội chứng Guillain-Barré (GBS) được báo cáo trong thai kỳ và thời kỳ hậu sản.
Có thể bạn quan tâm
-
Vượt ra ngoài chứng ngứa liên quan đến bệnh thận mãn tính (CKD): Ngứa cận ung thư làm lộ diện bệnh CLL/SLL ở bệnh nhân suy thận giai đoạn cuối (ESRD): Báo cáo ca bệnh
Beyond CKD-Associated Pruritus: Paraneoplastic Itch Revealing CLL/SLL in ESRD: A Case Report
-
Thay thế bác sĩ bằng điều dưỡng trong môi trường bệnh viện: Hiệu quả đối với kết cục của bệnh nhân, quy trình chăm sóc và chi phí
Nurse-physician substitution in hospital settings: Effects on patient outcomes, care processes, and costs
-
Kháng thể đơn dòng nhắm mục tiêu protein amyloid-beta cho người bị suy giảm nhận thức nhẹ hoặc sa sút trí tuệ nhẹ do bệnh Alzheimer
Amyloid-beta-targeting monoclonal antibodies for people with mild cognitive impairment or mild dementia due to Alzheimer’s disease
-
Chiến dịch Bangui: Câu chuyện về máu, khoa học và sự khai thác y sinh học
The Bangui operation: A story of blood, science and biomedical exploitation