Chủ đề lâm sàng
Liệu pháp miễn dịch kết hợp hóa trị so với hóa trị đơn thuần trong điều trị ung thư vú thể tam âm giai đoạn sớm
Immunotherapy plus chemotherapy versus chemotherapy alone for early triple-negative breast cancer
Dontbemed Brief Review
Adding pembrolizumab to neoadjuvant chemotherapy followed by adjuvant pembrolizumab significantly improves pathological complete response (pCR), event-free survival (EFS), and overall survival (OS) in stage II–III triple-negative breast cancer (TNBC), and is the current standard of care. In contrast, adding immunotherapy only in the postoperative (adjuvant-only) setting has not demonstrated benefit.
Việc bổ sung pembrolizumab vào hóa trị tân bổ trợ, sau đó tiếp tục sử dụng pembrolizumab bổ trợ giúp cải thiện đáng kể tỷ lệ đáp ứng hoàn toàn trên mô bệnh học (pCR), thời gian sống sót không gặp biến cố (EFS) và tỷ lệ sống sót tổng thể (OS) ở bệnh nhân ung thư vú thể tam âm (TNBC) giai đoạn II–III, và đây là tiêu chuẩn chăm sóc hiện hành. Ngược lại, việc bổ sung liệu pháp miễn dịch chỉ trong giai đoạn sau phẫu thuật (chỉ bổ trợ) đã không chứng minh được lợi ích.
Neoadjuvant immunotherapy + chemotherapy (before surgery)
Liệu pháp miễn dịch tân bổ trợ + hóa trị (trước phẫu thuật)
The landmark KEYNOTE-522 trial (n = 1,174; stage II–III TNBC) established the paradigm. Patients received neoadjuvant pembrolizumab + carboplatin/paclitaxel → doxorubicin or epirubicin/cyclophosphamide + pembrolizumab, followed by adjuvant pembrolizumab for up to 9 cycles after surgery: 1 2
Thử nghiệm lâm sàng mang tính cột mốc KEYNOTE-522 (n = 1.174; TNBC giai đoạn II–III) đã thiết lập mô hình điều trị này. Bệnh nhân được điều trị bằng pembrolizumab tân bổ trợ + carboplatin/paclitaxel → doxorubicin hoặc epirubicin/cyclophosphamide + pembrolizumab, tiếp theo là pembrolizumab bổ trợ lên đến 9 chu kỳ sau phẫu thuật: 1 2
- pCR rate: 64.8% vs. 51.2% (difference 13.6 percentage points; P < 0.001) 1
- EFS at 5 years: ~81% vs. ~72% (HR 0.65; 35% relative risk reduction), with benefit sustained at median follow-up of 75.1 months 2 3
- OS at 5 years: 86.6% vs. 81.7% (HR for death, P = 0.002), a 4.9 percentage-point absolute improvement 2
- Tỷ lệ pCR: 64,8% so với 51,2% (chênh lệch 13,6 điểm phần trăm; P kém hơn 0,001) 1
- EFS tại thời điểm 5 năm: ~81% so với ~72% (HR 0,65; giảm 35% nguy cơ tương đối), với lợi ích được duy trì ổn định ở thời gian theo dõi trung vị là 75,1 tháng 2 3
- OS tại thời điểm 5 năm: 86,6% so với 81,7% (HR đối với tử vong, P = 0,002), một sự cải thiện tuyệt đối 4,9 điểm phần trăm 2
Neoadjuvant pembrolizumab combined with chemotherapy followed by adjuvant pembrolizumab resulted in a significant improvement, as compared with neoadjuvant chemotherapy alone, in overall survival among patients with previously untreated, high-risk, early-stage triple-negative breast cancer.
— Peter Schmid, M. D., et al., Queen Mary University London and other institutions
Pembrolizumab tân bổ trợ kết hợp với hóa trị, tiếp theo là pembrolizumab bổ trợ đã giúp cải thiện đáng kể tỷ lệ sống sót tổng thể so với chỉ dùng hóa trị tân bổ trợ đơn thuần ở những bệnh nhân mắc ung thư vú thể tam âm giai đoạn sớm, nguy cơ cao, chưa từng được điều trị trước đây.
— Bác sĩ Peter Schmid, và cộng sự, Đại học Queen Mary London và các tổ chức khác
The benefit was observed regardless of PD-L1 expression status, nodal involvement, or tumor size, though subgroup analyses are underpowered and require cautious interpretation 2 3. The IMpassion031 trial similarly showed that neoadjuvant atezolizumab + nab-paclitaxel/doxorubicin-cyclophosphamide significantly improved pCR (58% vs. 41%; P = 0.0044) irrespective of PD-L1 status 4.
Lợi ích này được ghi nhận bất kể trạng thái biểu hiện PD-L1, tình trạng di căn hạch hay kích thước khối u, mặc dù các phân tích nhóm phụ chưa đủ mạnh và cần được diễn giải một cách thận trọng 2 3. Thử nghiệm IMpassion031 tương tự cũng cho thấy atezolizumab tân bổ trợ + nab-paclitaxel/doxorubicin-cyclophosphamide làm cải thiện đáng kể tỷ lệ pCR (58% so với 41%; P = 0,0044) không phụ thuộc vào trạng thái PD-L1 4.
A 2026 Cochrane systematic review (7 RCTs, 4,341 participants) confirmed that PD-1/PD-L1 inhibitors combined with neoadjuvant chemotherapy probably improve pCR (RR 1.47), EFS (HR 0.64), and OS (HR 0.56) compared with chemotherapy alone, with moderate-to-high certainty evidence 5.
Một tổng quan hệ thống Cochrane năm 2026 (7 nghiên cứu RCT, 4.341 người tham gia) đã xác nhận rằng các chất ức chế PD-1/PD-L1 kết hợp với hóa trị tân bổ trợ có khả năng cải thiện pCR (RR 1,47), EFS (HR 0,64) và OS (HR 0,56) so với hóa trị đơn thuần, với bằng chứng có độ tin cậy từ trung bình đến cao 5.

Adjuvant-only immunotherapy (after surgery)
Liệu pháp miễn dịch chỉ bổ trợ (sau phẫu thuật)
The ALEXANDRA/IMpassion030 trial (n = 2,199; stage II–III TNBC) tested adding atezolizumab to standard adjuvant chemotherapy in patients who underwent surgery first (without neoadjuvant immunotherapy). The results were negative: invasive DFS HR 1.11 (95% CI 0.87–1.42; P = 0.38), with no benefit in OS or any secondary endpoint 6. This trial is the only phase 3 study evaluating a purely adjuvant checkpoint inhibitor approach in early TNBC, and its findings do not support this strategy.
Thử nghiệm ALEXANDRA/IMpassion030 (n = 2.199; TNBC giai đoạn II–III) đã đánh giá việc bổ sung atezolizumab vào hóa trị bổ trợ tiêu chuẩn ở những bệnh nhân được phẫu thuật trước (không dùng liệu pháp miễn dịch tân bổ trợ). Các kết quả thu được là tiêu cực (không có hiệu quả): HR của thời gian sống sót không bệnh xâm lấn (DFS) là 1,11 (KTC 95% 0,87–1,42; P = 0,38), và không mang lại lợi ích nào đối với OS hoặc bất kỳ kết cục phụ nào 6. Thử nghiệm này là nghiên cứu pha 3 duy nhất đánh giá hướng tiếp cận chất ức chế điểm kiểm soát miễn dịch thuần túy bổ trợ trong ung thư vú thể tam âm giai đoạn sớm, và các phát hiện của nó không ủng hộ chiến lược này.
Safety considerations
Các cân nhắc về tính an toàn
Across trials, adding immunotherapy to chemotherapy increases immune-related serious adverse events (OR ~1.75), most commonly endocrine disorders (hypothyroidism, adrenal insufficiency, thyroiditis) and pneumonitis 5 7. Grade ≥3 immune-mediated adverse events occurred in ~13% with pembrolizumab vs. ~1% with placebo in KEYNOTE-522 7. Overall rates of any adverse events and treatment-related deaths were not significantly different between groups, though treatment discontinuation was higher with immunotherapy (27.7% vs. 14.1%) 7 8.
Qua các thử nghiệm, việc bổ sung liệu pháp miễn dịch vào hóa trị làm tăng các biến cố có hại nghiêm trọng liên quan đến miễn dịch (OR ~1,75), phổ biến nhất là các rối loạn nội tiết (suy giáp, suy tuyến thượng thận, viêm tuyến giáp) và viêm phổi kẽ 5 7. Các biến cố có hại qua trung gian miễn dịch độ lớn hơn hoặc bằng 3 xảy ra ở khoảng 13% bệnh nhân dùng pembrolizumab so với khoảng 1% ở nhóm dùng giả dược trong nghiên cứu KEYNOTE-522 7. Tỷ lệ tổng thể của bất kỳ biến cố có hại nào và tỷ lệ tử vong liên quan đến điều trị không có sự khác biệt ý nghĩa giữa các nhóm, mặc dù tỷ lệ ngừng điều trị cao hơn ở nhóm dùng liệu pháp miễn dịch (27,7% so với 14,1%) 7 8.
Current guideline recommendations
Khuyến cáo từ hướng dẫn hiện hành
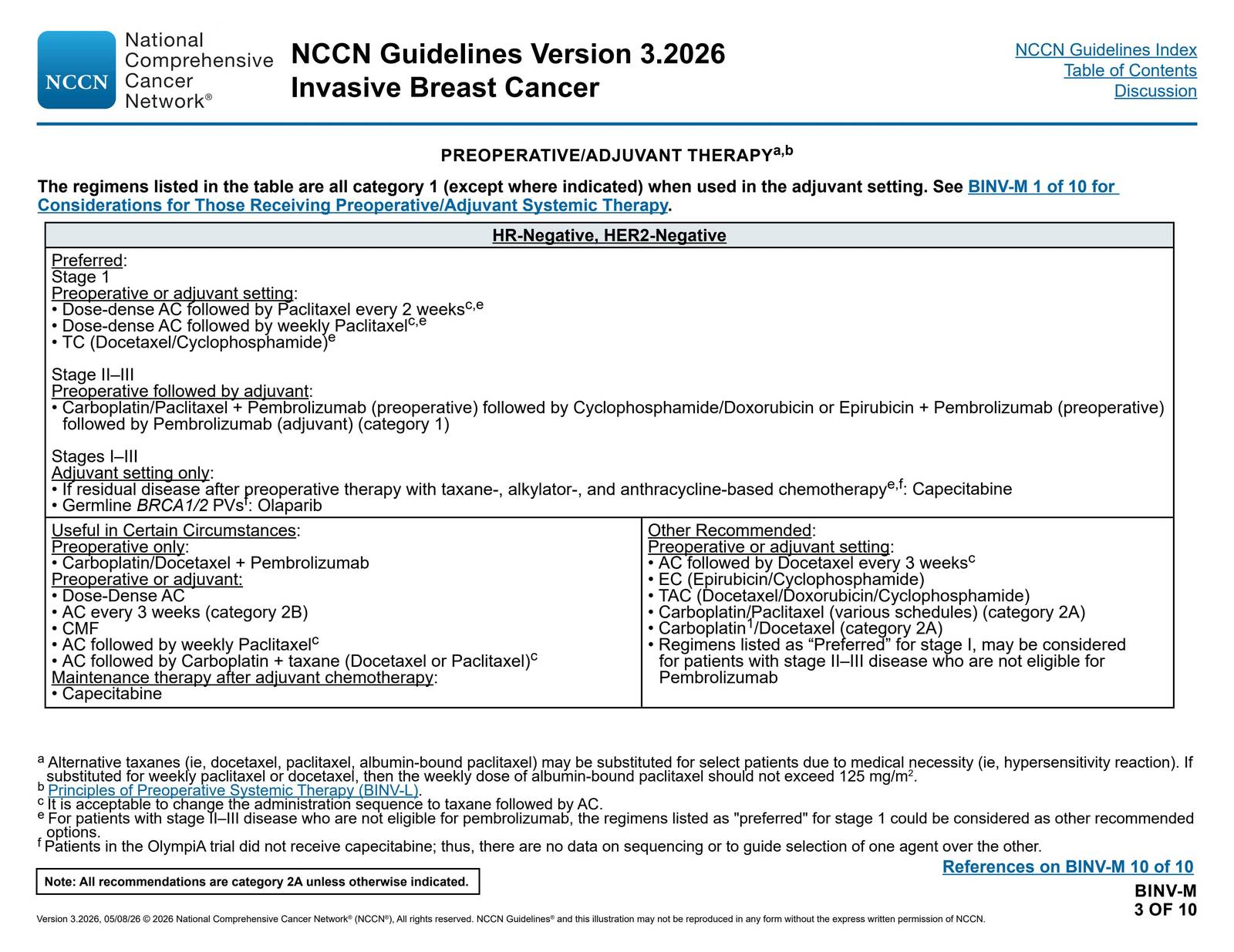
The NCCN Breast Cancer Guidelines (v3.2026) list neoadjuvant pembrolizumab + carboplatin/paclitaxel → AC/EC + pembrolizumab → adjuvant pembrolizumab as the preferred, category 1 regimen for stage II–III HR-negative, HER2-negative breast cancer 9. The ASCO Guideline Rapid Recommendation Update similarly endorses this approach 7. For stage I disease, standard chemotherapy without pembrolizumab remains preferred.
Hướng dẫn Điều trị Ung thư Vú của NCCN (phiên bản v3.2026) xếp phác đồ pembrolizumab tân bổ trợ + carboplatin/paclitaxel → AC/EC + pembrolizumab → pembrolizumab bổ trợ là phác đồ được ưu tiên, danh mục 1 (category 1) đối với ung thư vú giai đoạn II–III có thụ thể nội tiết âm tính (HR-negative) và HER2 âm tính (HER2-negative) 9. Bản Cập nhật Khuyến cáo Nhanh của Hướng dẫn ASCO tương tự cũng đồng thuận với hướng tiếp cận này 7. Đối với bệnh giai đoạn I, hóa trị tiêu chuẩn không kết hợp pembrolizumab vẫn là lựa chọn được ưu tiên hơn.
Key takeaway
Thông điệp cốt lõi
The timing of immunotherapy relative to surgery is critical. The neoadjuvant-through-adjuvant strategy (starting pembrolizumab before surgery and continuing after) produces durable improvements in pCR, EFS, and OS. Adding immunotherapy only after surgery does not improve outcomes and adds toxicity.
Thời điểm sử dụng liệu pháp miễn dịch so với thời điểm phẫu thuật đóng vai trò cực kỳ then chốt. Chiến lược xuyên suốt từ tân bổ trợ đến bổ trợ (bắt đầu dùng pembrolizumab trước phẫu thuật và tiếp tục sau phẫu thuật) mang lại những cải thiện bền vững về pCR, EFS và OS. Việc chỉ bổ sung liệu pháp miễn dịch sau phẫu thuật không giúp cải thiện kết cục lâm sàng mà còn làm tăng thêm độc tính.
Reference
- Schmid, P., Cortes, J., Pusztai, L., et al. (2020). Pembrolizumab for Early Triple-Negative Breast Cancer. The New England Journal of Medicine.
- Schmid, P., Cortes, J., Dent, R., et al. (2024). Overall Survival with Pembrolizumab in Early-Stage Triple-Negative Breast Cancer. The New England Journal of Medicine.
- Schmid, P., Cortes, J., Dent, R., et al. (2022). Event-free Survival with Pembrolizumab in Early Triple-Negative Breast Cancer. The New England Journal of Medicine.
- Mitendorf, E. A., Zhang, H., Barrios, C. H., et al. (2020). Neoadjuvant Atezolizumab in Combination With Sequential Nab-Paclitaxel and Anthracycline-Based Chemotherapy Versus Placebo and Chemotherapy in Patients With Early-Stage Triple-Negative Breast Cancer (IMpassion031): A Randomised, Double-Blind, Phase 3 Trial. Lancet.
- Gao, Y., Liu, M., Li, L., et al. (2026). Immune Checkpoint Inhibitors and Chemotherapy Versus Chemotherapy for Early Triple-Negative Breast Cancer. The Cochrane Database of Systematic Reviews.
- Ignatiadis, M., Bailey, A., McArthur, H., et al. (2025). Adjuvant Atezolizumab for Early Triple-Negative Breast Cancer: The ALEXANDRA/IMpassion030 Randomized Clinical Trial. The Journal of the American Medical Association.
- Korde, L. A., Somerfield, M. R., Hershman, D. L., & Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer Guideline Expert Panel. (2022). Use of Immune Checkpoint Inhibitor Pembrolizumab in the Treatment of High-Risk, Early-Stage Triple-Negative Breast Cancer: ASCO Guideline Rapid Recommendation Update. Journal of Clinical Oncology.
- Shah, M., Osgood, C. L., Amatya, A. K., et al. (2022). FDA Approval Summary: Pembrolizumab for Neoadjuvant and Adjuvant Treatment of Patients With High-Risk Early-Stage Triple-Negative Breast Cancer. Clinical Cancer Research.
- National Comprehensive Cancer Network. (2026). Breast Cancer (v3.2026).
Chủ đề Lâm sàng
-
Hiệu quả của các can thiệp kích thích hoặc phản hồi sinh học trong kiểm soát tình trạng mệt mỏi sau chấn thương sọ não (TBI)
Effects of stimulation or biofeedback interventions for fatigue management after traumatic brain injury (TBI)
-
Hóa trị qua đường động mạch (IAC) so với hóa trị qua đường tĩnh mạch (IVC) ở trẻ em mắc u nguyên bào võng mạc: Lợi ích, tác hại và liệu pháp phối hợp
Intra‐arterial chemotherapy (IAC) versus intravenous chemotherapy (IVC) for children with retinoblastoma: Benefits, harms, and combination therapy
-
Theo dõi liên tục bằng quang phổ cận hồng ngoại (NIRS) não ở trẻ sinh rất non: Lợi ích và tác hại
Continuous cerebral near‐infrared spectroscopy (NIRS) monitoring monitoring in very preterm infants: Benefits and harms
Bằng chứng mới
Ca lâm sàng
-
Yếu toàn thể do Hạ calci máu và Giảm phosphate máu từ ức chế acid mạnh
Generalized Weakness Due to Hypocalcemia and Hypophosphatemia From Potent Acid Suppression
-
Tắc động mạch cảnh nội tiến triển trong bệnh liên quan IgG4: Báo cáo ca bệnh và tổng quan tài liệu
Progressive Internal Carotid Artery Occlusion in IgG4-Related Disease: A Case Report and Literature Review
-
Bệnh Kikuchi–Fujimoto Trình bày với Bệnh hạch bạch huyết mạc treo và Bệnh mô bào lympho thực bào máu ở một nam giới da đen trẻ tuổi
Kikuchi–Fujimoto Disease Presenting With Mesenteric Lymphadenopathy and Partial Hemophagocytic Lymphohistiocytosis in a Young Black Man
Y tế thế giới
-
Vape hương liệu gây ra sự xáo trộn lớn tại FDA – 3 nhà phân tích chính sách y tế giải thích khoa học đằng sau các sản phẩm gây tranh cãi
Flavored vapes led to a major shake-up at the FDA – 3 health policy analysts explain the science behind the controversial products
-
Việc siết chặt gian lận Medicaid của Trump nghe có vẻ hợp lý, nhưng nó có thể gây hại cho những người Mỹ cần chăm sóc dài hạn.
Trump’s Medicaid fraud crackdown may sound sensible, but it could harm Americans who require long-term care
-
Tiêm vắc-xin cúm có bị cúm không? 5 câu hỏi về vắc-xin được giải đáp
Does the flu vaccine give you the flu? 5 questions about the vaccine answered