Ca lâm sàng
Nhiễm trùng vắc-xin Bacillus Calmette-Guérin lan tỏa tiến triển nhanh (Viêm hạch BCG) ở trẻ sơ sinh 3 tháng tuổi không có suy giảm miễn dịch: Báo cáo ca bệnh
Rapidly Progressive Disseminated Bacillus Calmette-Guérin Infection (BCGitis) in a 3-Month-Old Infant Without Immunodeficiency: A Case Report


Abstract
Tóm tắt
BACKGROUND: Disseminated Bacillus Calmette-Guérin (BCG) disease is a rare but severe complication of BCG vaccination, particularly in immunocompromised children, and is associated with high mortality. The incidence of disseminated Bacillus Calmette-Guérin disease is approximately 1.56 to 4.29 cases per million vaccinated individuals, with an overall mortality of 60% to 80%. Lesions most commonly appear in the right arm, axilla, and areas adjacent to the injection site. We report a case of a rare presentation of disseminated BCGitis 3 months after the intradermal vaccine.
BỐI CẢNH: Bệnh lao BCG lan tỏa (Disseminated Bacillus Calmette-Guérin disease) là một biến chứng hiếm gặp nhưng nghiêm trọng sau khi tiêm vắc-xin BCG, đặc biệt là ở trẻ suy giảm miễn dịch, và có tỷ lệ tử vong cao. Tần suất mắc bệnh lao BCG lan tỏa là khoảng 1,56 đến 4,29 ca trên một triệu người được tiêm chủng, với tỷ lệ tử vong chung từ 60% đến 80%. Các tổn thương thường xuất hiện nhất ở tay phải, nách và các vùng lân cận vị trí tiêm. Chúng tôi báo cáo một trường hợp có biểu hiện hiếm gặp của viêm hạch BCG lan tỏa (disseminated BCGitis) xảy ra 3 tháng sau khi tiêm vắc-xin trong da.
CASE REPORT: A previously healthy 3-month-old infant developed devastating skin, subcutaneous, bone, lymphatic, and systemic complications located in the head and neck. The rapidly progressive and destructive growth of the lesions simulated a malignant neoplasm. After several weeks of investigation and challenging diagnosis, the patient was successfully treated with a 7-month regimen of rifampicin, isoniazid, and ethambutol, with resolution and no sequelae. No underlying immunodeficiency was identified. At 3-year follow-up, the child demonstrated normal neurodevelopment and psychomotor function, with no significant infections or other immune-related problems.
BÁO CÁO CA BỆNH: Một trẻ sơ sinh 3 tháng tuổi trước đó khỏe mạnh đã tiến triển các biến chứng nặng nề ở da, mô dưới da, xương, hệ bạch huyết và toàn thân khu trú ở vùng đầu cổ. Sự phát triển nhanh chóng và mang tính phá hủy của các tổn thương này giả lập một khối u ác tính. Sau vài tuần khảo sát và chẩn đoán đầy thách thức, bệnh nhân đã được điều trị thành công bằng phác đồ 7 tháng gồm rifampicin, isoniazid và ethambutol, bệnh thuyên giảm hoàn toàn và không để lại di chứng. Không tìm thấy tình trạng suy giảm miễn dịch tiềm ẩn nào. Tại thời điểm theo dõi sau 3 năm, trẻ cho thấy sự phát triển thần kinh và chức năng tâm thần vận động bình thường, không bị nhiễm trùng nghiêm trọng hoặc gặp các vấn đề khác liên quan đến miễn dịch.
CONCLUSIONS: Disseminated BCGitis can be the first manifestation of a primary immunodeficiency or secondary immunodeficiency or can occur sporadically, as in our patient. The condition can progress rapidly and be fatal, making early recognition essential.
KẾT LUẬN: Viêm hạch BCG lan tỏa có thể là biểu hiện đầu tiên của tình trạng suy giảm miễn dịch bẩm sinh (nguyên phát) hoặc suy giảm miễn dịch mắc phải (thứ phát), hoặc có thể xảy ra đơn phát như ở bệnh nhân của chúng tôi. Tình trạng này có thể tiến triển nhanh chóng và dẫn đến tử vong, do đó việc phát hiện sớm là vô cùng thiết yếu.
Keywords: BCG vaccine, immune system, isoniazid, Mycobacterium, temporal bone
Từ khóa: vắc-xin BCG, hệ miễn dịch, isoniazid, Mycobacterium, xương thái dương
Introduction
Đặt vấn đề
The tuberculosis (TB) vaccine, Bacillus Calmette-Guérin (BCG), is a live attenuated bacilli of Mycobacterium bovis, which recommended for all newborns, unless there are specific contraindications 1. When BCG vaccine is applied intradermally, it causes an artificial primary infection that aims to develop a specific immune response to control a future bacilli infection 2. The World Health Organization recommends BCG vaccination in all neonates in those areas with a high prevalence of TB, which includes Brazil and more than 150 countries. Since 1976, all Brazilian newborns have received the vaccine in the maternity ward, and there have been minimal adverse reactions 3. The incidence of adverse BCG reactions is very low, yet may be underestimated, related to the benignity of most cases 4. Overall, BCG vaccine-associated adverse reactions occur as a result of vaccine strain modifications, administration techniques, viable bacillary batch load, and, most importantly, host characteristics – primarily immune function. Reactions include fever, subcutaneous abscess, keloids, skin lesions at the vaccination site, and severe lymphadenitis. Osteitis and osteomyelitis are uncommon. The complications and adverse reactions of BCG vaccination have been reported in 310 cases per million vaccinated individuals and include lymphadenitis, persistent ulcer, and remote infection. The rarest complication is disseminated BCG disease, with an incidence of approximately 1.56 to 4.29 cases per million vaccinations, which leads to serious complications and has an overall mortality rate of 60% to 80% 5,6. Hesseling et al proposed phenotypes to BCG-induced disease based on a revised pediatric classification, designated as: local, regional, distant, or disseminated patterns. The diagnosis can be confirmed by clinical course, dermatological features, pathology, specific polymerase chain reaction (PCR), and spoligotyping 7. Disseminated (or systemic) BCGitis is an infection caused by BCG that progresses with hematogenous or distant lymphatic spread, causing septicemia and involving the lymph nodes, bones, or systemic organs distant from the vaccine injection site, such as lung involvement, splenomegaly, enteropathy. BCGitis is the most severe adverse effect of the BCG vaccine and can lead to severe sepsis and death if left untreated 8. When BCGitis affects the ear and parotid gland, it can become even more tragic, due to the risk of deafness, paralysis of the facial nerve, dizziness, meningitis, and invasion of the central nervous system due to proximity to the lateral skull base.
Vắc-xin phòng bệnh lao (TB), Bacillus Calmette-Guérin (BCG), là một loại trực khuẩn sống giảm độc lực của Mycobacterium bovis, được khuyến cáo cho tất cả trẻ sơ sinh, trừ khi có các chống chỉ định cụ thể 1. Khi vắc-xin BCG được tiêm trong da, nó gây ra một đợt nhiễm trùng sơ nhiễm nhân tạo nhằm mục đích phát triển một đáp ứng miễn dịch đặc hiệu để kiểm soát tình trạng nhiễm trực khuẩn trong tương lai 2. Tổ chức Y tế Thế giới khuyến cáo tiêm vắc-xin BCG cho tất cả trẻ sơ sinh tại những khu vực có tỷ lệ mắc bệnh lao cao, bao gồm Brazil và hơn 150 quốc gia khác. Kể từ năm 1976, tất cả trẻ sơ sinh tại Brazil đều được tiêm vắc-xin này tại khoa sản và ghi nhận rất ít phản ứng bất lợi 3. Tỷ lệ xảy ra các phản ứng bất lợi do BCG là rất thấp, tuy nhiên có thể đang bị đánh giá thấp hơn thực tế do tính chất lành tính của hầu hết các trường hợp 4. Nhìn chung, các phản ứng bất lợi liên quan đến vắc-xin BCG xảy ra do sự biến đổi chủng vắc-xin, kỹ thuật tiêm, hàm lượng trực khuẩn sống trong lô vắc-xin, và quan trọng nhất là các đặc điểm của vật chủ – chủ yếu là chức năng miễn dịch. Các phản ứng bao gồm sốt, áp-xe dưới da, sẹo lồi, tổn thương da tại vị trí tiêm và viêm hạch bạch huyết nghiêm trọng. Viêm xương và viêm tủy xương là những trường hợp không phổ biến. Các biến chứng và phản ứng bất lợi của việc tiêm vắc-xin BCG đã được báo cáo trong 310 ca trên một triệu người được tiêm chủng, bao gồm viêm hạch, loét dai dẳng và nhiễm trùng ở xa. Biến chứng hiếm gặp nhất là bệnh lao BCG lan tỏa, với tỷ lệ lưu hành khoảng 1,56 đến 4,29 ca trên một triệu lượt tiêm chủng, dẫn đến các biến chứng nghiêm trọng và có tỷ lệ tử vong chung từ 60% đến 80% 5,6. Hesseling và các cộng sự đã đề xuất các kiểu hình đối với bệnh do BCG gây ra dựa trên một phân loại nhi khoa đã được sửa đổi, được chỉ định thành các dạng: khu trú, vùng, ở xa, hoặc lan tỏa. Việc chẩn đoán có thể được xác định bằng diễn tiến lâm sàng, đặc điểm da liễu, bệnh lý học, phản ứng chuỗi polymerase (PCR) đặc hiệu và định tuýp phân tử spoligotyping 7. Viêm hạch BCG lan tỏa (hoặc hệ thống) là một tình trạng nhiễm trùng do BCG tiến triển thông qua đường máu hoặc đường bạch huyết ở xa, gây nhiễm trùng huyết và ảnh hưởng đến các hạch bạch huyết, xương hoặc các cơ quan nội tạng ở xa vị trí tiêm vắc-xin, chẳng hạn như tổn thương phổi, lách to, bệnh lý ruột. Viêm hạch BCG là tác dụng bất lợi nghiêm trọng nhất của vắc-xin BCG và có thể dẫn đến nhiễm trùng huyết nặng và tử vong nếu không được điều trị 8. Khi viêm hạch BCG ảnh hưởng đến tai và tuyến mang tai, tình trạng này có thể trở nên tồi tệ hơn do nguy cơ điếc, liệt dây thần kinh mặt, chóng mặt, viêm màng não và xâm nhập vào hệ thần kinh trung ương do vị trí nằm gần nền sọ bên.
The presentation forms of BCGitis can be recognized in its natural evolution. Non-suppurative BCGitis occurs earlier and usually resolves spontaneously within a few weeks without any sequelae. In some cases, the affected ganglion progressively increases in size and develops suppuration, swelling, and erythema of the underlying skin. Suppurative BCGitis can develop after 2 to 4 months of BCG vaccination and persist for several months. BCGitis occurrence is most commonly secondary to immune deficiency, especially primary immunodeficiency 6,7. We report a case of a previously healthy patient without detected immune system deficiencies before the diagnosis. In our literature search, we did not find any reported cases of disseminated BCGitis affecting the ear, temporal bone, or parotid gland or simulating a neoplasm in the head and neck.
Các dạng biểu hiện của viêm hạch BCG có thể được nhận biết trong quá trình tiến triển tự nhiên của nó. Viêm hạch BCG không mủ xuất hiện sớm hơn và thường tự khỏi trong vòng vài tuần mà không để lại di chứng. Trong một số trường hợp, hạch bị tổn thương tăng dần kích thước và tiến triển thành mủ, sưng tấy và ban đỏ ở vùng da bên dưới. Viêm hạch BCG hóa mủ có thể phát triển sau 2 đến 4 tháng tiêm vắc-xin BCG và kéo dài trong vài tháng. Sự xuất hiện của viêm hạch BCG thường là thứ phát sau tình trạng suy giảm miễn dịch, đặc biệt là suy giảm miễn dịch bẩm sinh 6,7. Chúng tôi báo cáo một trường hợp bệnh nhân trước đó khỏe mạnh và không phát hiện thấy tình trạng suy giảm hệ miễn dịch nào trước khi chẩn đoán. Trong quá trình tìm kiếm tài liệu y văn, chúng tôi không tìm thấy bất kỳ trường hợp nào được báo cáo về viêm hạch BCG lan tỏa ảnh hưởng đến tai, xương thái dương, tuyến mang tai hoặc giả lập một khối u ở vùng đầu cổ.
Case Report
Báo cáo ca bệnh
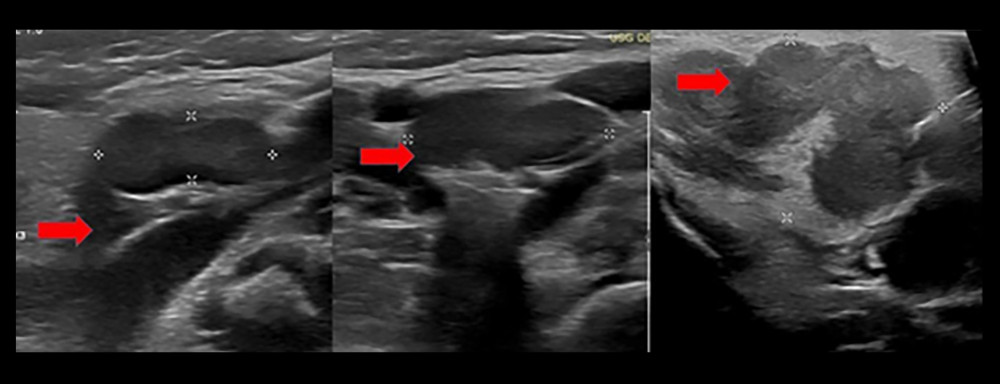
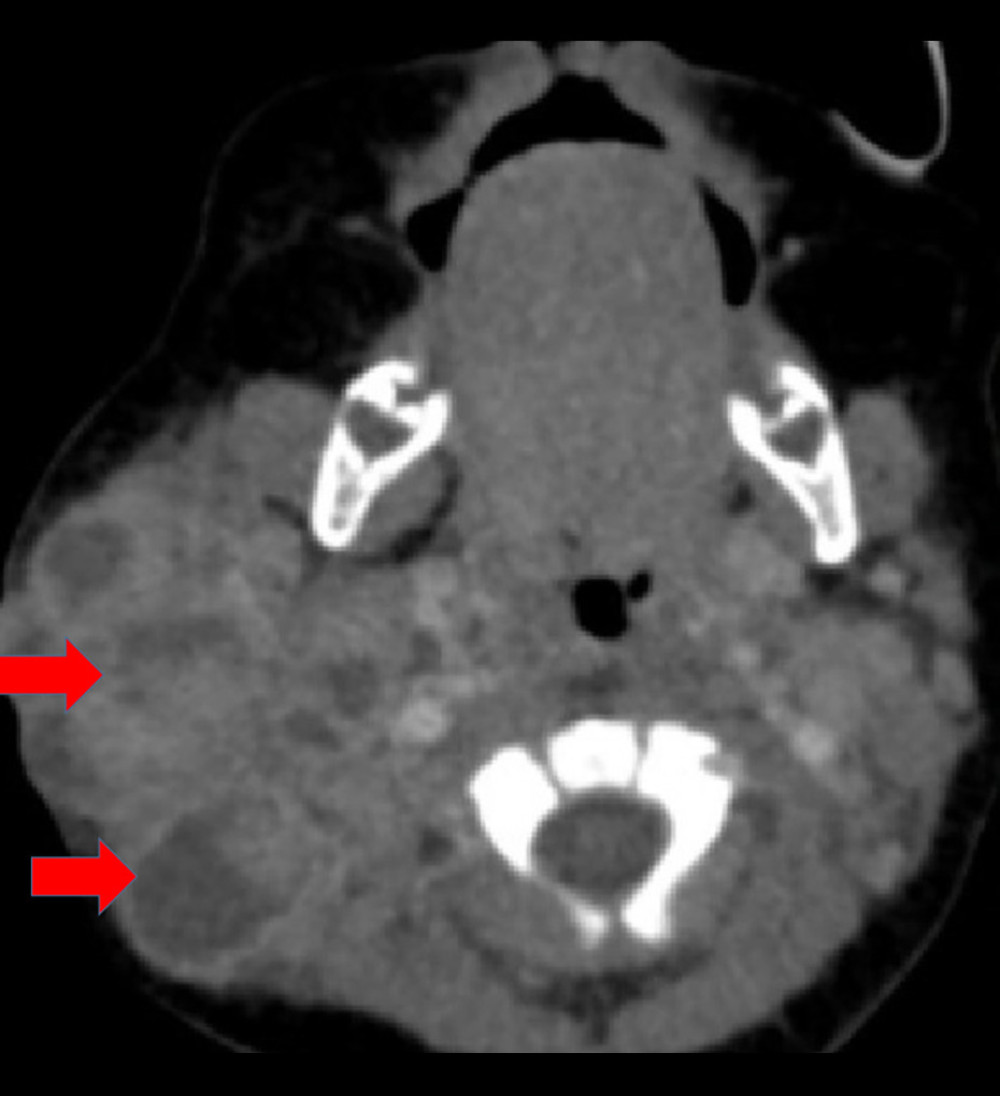
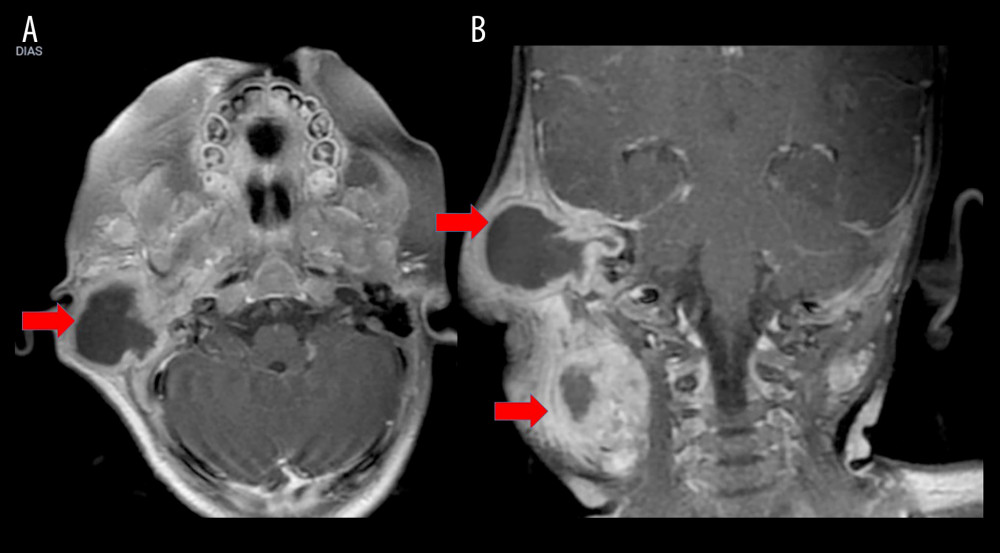
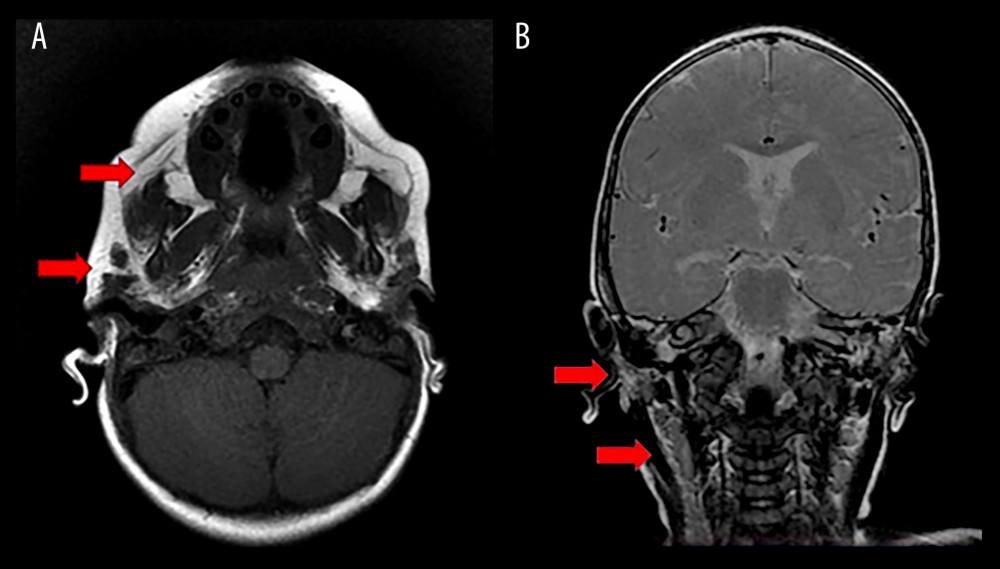
A previously healthy 3-month-old male infant presented with a daily purulent otorrhea unilaterally in the right ear for 1 month, which was refractory to oral antibiotic therapy. This was associated with high fever, irritability, prostration, and weight loss. Even with the administration of broad-spectrum antibiotics, after 1 week of hospitalization, the patient developed progressive growth of an infra-auricular and right retroauricular cervical mass. The mass continued to enlarge and, 2 weeks later, measured approximately 2.5×2.0 cm with phlogosis and a drainage point, in addition to ipsilateral suppurative lymphadenitis. There was associated ipsilateral axillary lymphadenopathy. In the third week, the lesion evolved with an ulcerative-vegetative appearance (Figure 1). Ultrasound examination revealed lymph node enlargement and a lymph node conglomerate at right level II with loss of hilar morphology, measuring 2.6×1.5 cm in its largest axial dimensions. Lymph nodes increased in number, with some enlarged and showing loss of fatty hila at right level IB and bilateral levels II, III, and V, with right-sided predominance. A heterogeneous solid nodule with irregular edges was present in the right retroauricular region, associated with apparent bone erosion of the adjacent mastoid, measuring approximately 2.2×2.1 cm. The right parotid gland was enlarged with heterogeneous echotexture and intraglandular lymph node enlargement (Figure 2). Computed tomography (CT) showed an expansive lesion of the degenerative granulomatous type, with bone involvement, including the tympanic tegmen, and lymph node enlargement (Figure 3). Nuclear magnetic resonance imaging (MRI) showed an expansive and infiltrative lesion in the right cervical region. There was no involvement of the central nervous system (Figure 4).
Một bé trai sơ sinh 3 tháng tuổi trước đó khỏe mạnh nhập viện với tình trạng chảy mủ tai hàng ngày ở một bên tai phải kéo dài trong 1 tháng, kháng với liệu pháp kháng sinh đường uống. Tình trạng này đi kèm với sốt cao, kích thích, đờ đẫn và sụt cân. Ngay cả khi được sử dụng kháng sinh phổ rộng, sau 1 tuần nhập viện, bệnh nhân vẫn tiến triển một khối vùng cổ dưới tai và sau tai phải tăng dần kích thước. Khối này tiếp tục to lên và 2 tuần sau đó có kích thước khoảng 2,5×2,0 cm kèm theo sưng nóng đỏ đau (viêm tấy) và một điểm rò mủ, bên cạnh tình trạng viêm hạch bạch huyết hóa mủ cùng bên. Bệnh nhân cũng có hạch nách cùng bên kèm theo. Vào tuần thứ ba, tổn thương tiến triển thành dạng loét-sùi (Figure 1). Kết quả siêu âm cho thấy có hạch to và một cụm hạch ở nhóm II bên phải bị mất cấu trúc rốn hạch, kích thước trục lớn nhất là 2,6×1,5 cm. Số lượng hạch tăng lên, một số hạch phì đại và mất rốn hạch mỡ ở nhóm IB bên phải và nhóm II, III, V hai bên, ưu thế ở bên phải. Một nốt đặc không đồng nhất với bờ không đều xuất hiện ở vùng sau tai phải, liên quan đến tình trạng tiêu xương rõ rệt của xương chũm lân cận, kích thước khoảng 2,2×2,1 cm. Tuyến mang tai phải phì đại với cấu trúc âm không đồng nhất và có hạch to bên trong tuyến (Figure 2). Chụp cắt lớp vi tính (CT) cho thấy một tổn thương lan rộng thuộc dạng u hạt thoái hóa, có xâm lấn xương bao gồm cả trần hòm nhĩ, và hạch to (Figure 3). Chụp cộng hưởng từ (MRI) cho thấy một tổn thương lan rộng và thâm nhiễm ở vùng cổ phải. Không có sự xâm lấn vào hệ thần kinh trung ương (Figure 4).
The patient was hospitalized, and a treatment regimen with large spectrum intravenous antibiotics and corticosteroid was initiated. However, the patient still had fever, abundant purulent secretion, increasing leukocytosis, and elevated inflammatory test results for more than 4 weeks. There were no relevant occurrences of neonatal or family history, except for the maternal report of syphilis treated during the pregnancy of the patient’s 6-year-older brother. There was no parental consanguinity. The patient received BCG and hepatitis B vaccinations at birth. Serology results for HIV, Toxoplasma gondii, Epstein-Barr virus, Paracoccidioides, Histoplasma, Aspergillus, Leishmania, Treponema pallidum, cytomegalovirus, herpes simplex and zoster viruses, rubella, and Bartonella henselae were negative. C-ank, P-ank, anticardiolipin antibodies, rheumatoid factor, antinuclear antibodies, protein and hemoglobin electrophoresis, and all rheumatologic tests were within normal limits. Total lymphocytes, natural killer cells, B and T cells, CD3, CD4, CD8, and CD19 counts were normal, and the CD4/CD8 ratio was unaltered. Serum immunoglobulin levels (IgG, IgA, IgM, and IgE) were within the reference range.
Bệnh nhân được điều trị nội trú và bắt đầu phác đồ điều trị bằng kháng sinh truyền tĩnh mạch phổ rộng kết hợp với corticosteroid. Tuy nhiên, bệnh nhân vẫn tiếp tục sốt, tiết nhiều dịch mủ, tăng bạch cầu và các kết quả xét nghiệm viêm tăng cao trong hơn 4 tuần. Tiền sử sản khoa và gia đình không ghi nhận điều gì đặc biệt, ngoại trừ báo cáo của người mẹ về việc từng điều trị bệnh giang mai trong thai kỳ của anh trai bệnh nhân (lớn hơn bệnh nhân 6 tuổi). Bố mẹ không có quan hệ huyết thống gần. Bệnh nhân đã được tiêm vắc-xin BCG và viêm gan B từ lúc sinh. Kết quả huyết thanh chẩn đoán HIV, Toxoplasma gondii, virus Epstein-Barr, Paracoccidioides, Histoplasma, Aspergillus, Leishmania, Treponema pallidum, cytomegalovirus, virus herpes simplex và zoster, rubella, và Bartonella henselae đều cho kết quả âm tính. Các xét nghiệm C-ANCA, P-ANCA, kháng thể kháng cardiolipin, yếu tố dạng thấp (RF), kháng thể kháng nhân (ANA), điện di protein và huyết sắc tố, cùng tất cả các xét nghiệm thấp khớp đều nằm trong giới hạn bình thường. Số lượng lympho bào tổng số, tế bào giết tự nhiên (NK), tế bào B và T, CD3, CD4, CD8, và CD19 đều bình thường, và tỷ lệ CD4/CD8 không bị thay đổi. Nồng độ immunoglobulin trong huyết thanh (IgG, IgA, IgM, và IgE) nằm trong khoảng tham chiếu.
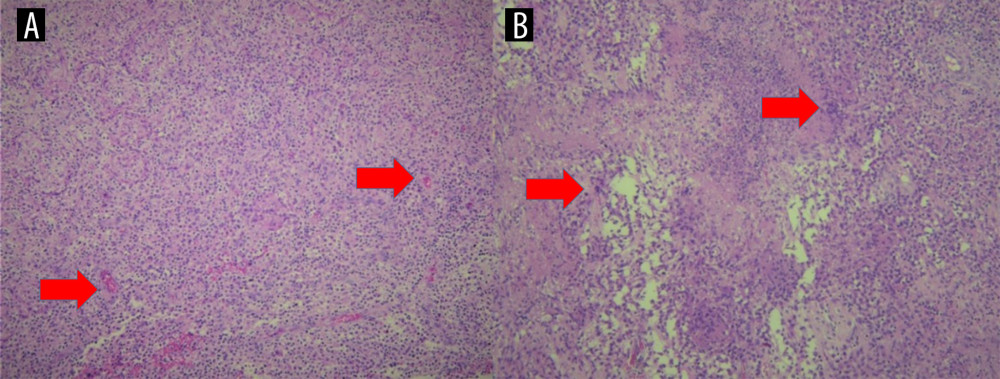
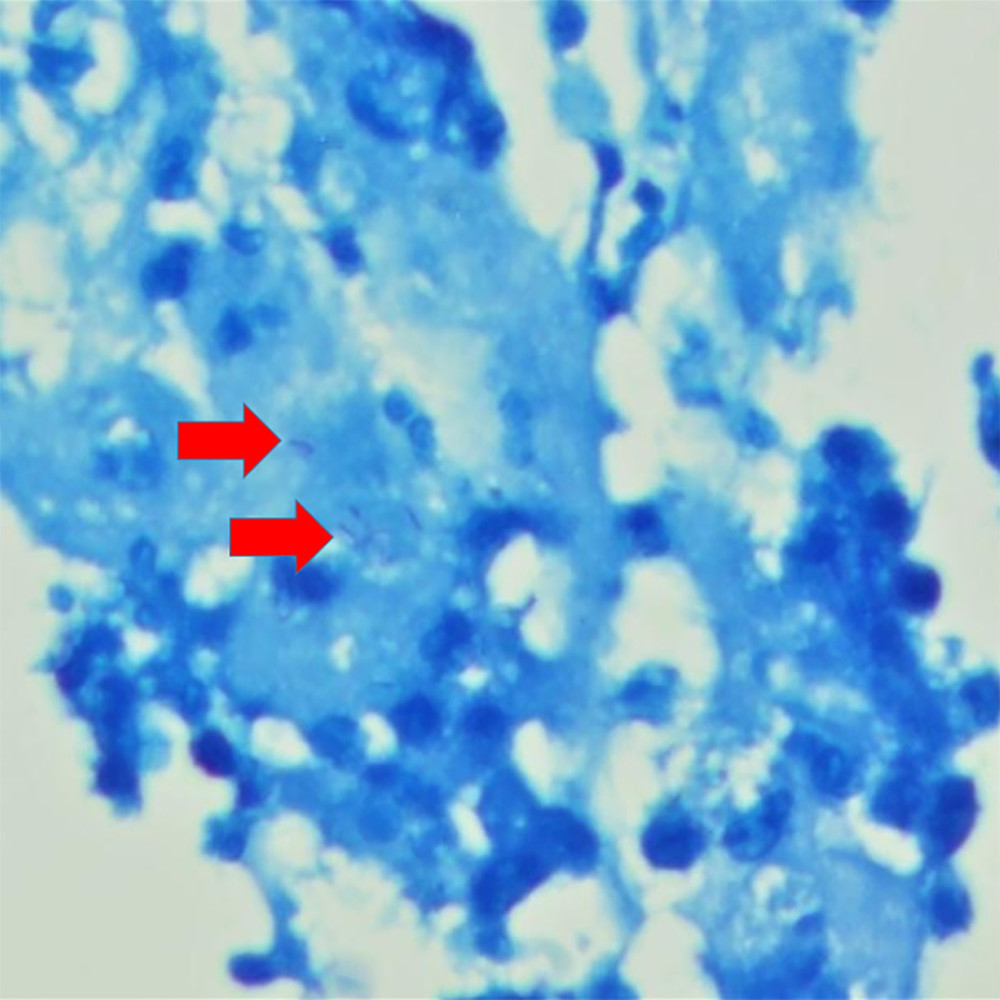
Despite all possible clinical measures and negative laboratory results, the patient’s condition continued to worsen, and we took him to the surgical center in the third week. The incisional biopsy of the lesion showed histiocytosis cells and multiple necrotizing granulomas (Figure 5), with the presence of Fite-Faraco-positive bacilliform structures, identifiable with acid-fast bacilli (Figure 6). M. bovis was isolated in the culture of the abscess secretion. The diagnosis of vaccine reaction to BCG was made, with disseminated infection by M. bovis. The treatment was established with rifampicin, isoniazid, and ethambutol (RIE) for 7 months, based on reports, case series, and literature reviews supporting this regimen as being well tolerated in children. All immunodeficiency screenings showed values within the reference range for serum immunoglobulin and lymphocyte subpopulation levels; the neutrophils oxidation test also showed no changes. The patient became afebrile from the first 3 days of therapy with the RIE regimen and had complete recovery at the end of treatment. MRI at 11 months after the diagnosis showed a complete resolution of the lesions, and lymph nodes disappeared (Figure 7).
Mặc dù đã áp dụng mọi biện pháp lâm sàng có thể và các kết quả xét nghiệm đều âm tính, tình trạng của bệnh nhân vẫn tiếp tục chuyển biến xấu, và chúng tôi đã đưa trẻ đến trung tâm phẫu thuật vào tuần thứ ba. Kết quả sinh thiết mở của tổn thương cho thấy các tế bào mô bào và nhiều u hạt hoại tử (Figure 5), với sự hiện diện của các cấu trúc dạng trực khuẩn dương tính với nhuộm Fite-Faraco, có thể định danh là trực khuẩn kháng kháng toan (Figure 6). M. bovis đã được phân lập trong môi trường nuôi cấy dịch mủ áp-xe. Chẩn đoán phản ứng vắc-xin với BCG đã được thiết lập, kèm theo nhiễm trùng lan tỏa do M. bovis. Việc điều trị được chỉ định bằng rifampicin, isoniazid và ethambutol (RIE) trong 7 tháng, dựa trên các báo cáo, chuỗi ca bệnh và các tổng quan tài liệu y văn ủng hộ phác đồ này vì được dung nạp tốt ở trẻ em. Tất cả các xét nghiệm tầm soát suy giảm miễn dịch đều cho giá trị trong khoảng tham chiếu đối với nồng độ immunoglobulin huyết thanh và các phân nhóm lympho bào; xét nghiệm phản ứng oxy hóa của bạch cầu trung tính cũng không ghi nhận thay đổi. Bệnh nhân đã hết sốt ngay từ 3 ngày đầu tiên điều trị bằng phác đồ RIE và hồi phục hoàn toàn khi kết thúc liệu trình. Phim chụp MRI ở thời điểm 11 tháng sau khi chẩn đoán cho thấy tổn thương đã biến mất hoàn toàn và các hạch bạch huyết không còn nữa (Figure 7).
During the 3-year follow-up, the child presented normal neurodevelopment and psychomotor function and no other relevant infections or problems with the immune system. We do not find any immunosuppression or comorbidities. The 2 older brothers received the BCG vaccine at birth with no adverse reactions The affected area is well healed eleven months after treatment (Figure 8).
Trong suốt 3 năm theo dõi, trẻ có sự phát triển thần kinh và chức năng tâm thần vận động bình thường, không mắc các bệnh nhiễm trùng nghiêm trọng khác hoặc gặp vấn đề gì về hệ miễn dịch. Chúng tôi không tìm thấy bất kỳ tình trạng suy giảm miễn dịch hay bệnh đồng mắc nào. Hai người anh trai của trẻ đều được tiêm vắc-xin BCG lúc sinh và không gặp phản ứng bất lợi nào. Vùng bị tổn thương đã lành tốt ở thời điểm mười một tháng sau điều trị (Figure 8).
Discussion
Bàn luận
The BCG vaccine is derived from M. bovis and can cause BCG vaccine-associated adverse events, especially in those patients with primary immunodeficiency 9. Although rare, BAC vaccine-associated adverse events include several local and serious systemic complications. Clinical recognition of disseminated BCG infection, as either BCGosis or disseminated BCGitis, is difficult, and there are many reports of diagnoses made only during autopsy 10. BCGosis is a very devastating complication of BCG immunization in immunocompromised children 11,12. However, our patient presented without any immunosuppression, even after profound investigation. The most common age of clinical presentation is children younger than 12 months; however, these adverse events can occur from birth to 3 years of age. The rate of disseminated BCGitis incidence is approximately 0.06 to 3.4 cases per million vaccinated individuals and presents a high mortality rate, mainly in immunocompromised patients, with an overall mortality of 60% to 80% 13. BCGosis mainly occurs in adults with acquired immunodeficiency. It can develop in patients who undergo BCG therapy, including intra-renal or intravesical instillation of BCG for cancer. The most commonly reported immunodeficiencies include combined immunodeficiencies such as HIV infection in the AIDS phase, chronic granulomatous disease, complete DiGeorge syndrome, and Mendelian susceptibility to mycobacterial disease 12,13.
Vắc-xin BCG có nguồn gốc từ M. bovis và có thể gây ra các biến cố bất lợi liên quan đến vắc-xin BCG, đặc biệt là ở những bệnh nhân bị suy giảm miễn dịch bẩm sinh 9. Mặc dù hiếm gặp, các biến cố bất lợi liên quan đến vắc-xin BCG bao gồm một số biến chứng tại chỗ và biến chứng hệ thống (toàn thân) nghiêm trọng. Việc nhận biết trên lâm sàng tình trạng nhiễm trùng BCG lan tỏa, dưới dạng bệnh lao BCGosis hoặc viêm hạch BCG lan tỏa (disseminated BCGitis), là rất khó khăn, và có nhiều báo cáo về việc chẩn đoán chỉ được thực hiện trong quá trình khám nghiệm tử thi 10. Lao BCGosis là một biến chứng rất nặng nề của việc tiêm chủng BCG ở trẻ em bị suy giảm miễn dịch 11,12. Tuy nhiên, bệnh nhân của chúng tôi biểu hiện bệnh mà không có bất kỳ tình trạng suy giảm miễn dịch nào, ngay cả sau khi đã thực hiện khảo sát chuyên sâu. Độ tuổi biểu hiện lâm sàng phổ biến nhất là trẻ dưới 12 tháng tuổi; tuy nhiên, các biến cố bất lợi này có thể xảy ra từ khi sinh ra cho đến 3 tuổi. Tỷ lệ mắc viêm hạch BCG lan tỏa là khoảng 0,06 đến 3,4 ca trên một triệu người được tiêm chủng và có tỷ lệ tử vong cao, chủ yếu ở bệnh nhân suy giảm miễn dịch, với tỷ lệ tử vong chung từ 60% đến 80% 13. Lao BCGosis chủ yếu xảy ra ở người trưởng thành bị suy giảm miễn dịch mắc phải. Tình trạng này có thể tiến triển ở những bệnh nhân trải qua liệu pháp điều trị bằng BCG, bao gồm bơm BCG vào trong thận hoặc trong bàng quang để điều trị ung thư. Các tình trạng suy giảm miễn dịch được báo cáo phổ biến nhất bao gồm suy giảm miễn dịch phối hợp như nhiễm HIV trong giai đoạn AIDS, bệnh u hạt mạn tính, hội chứng DiGeorge hoàn toàn, và tính dễ mắc bệnh do mycobacterium di truyền theo định luật Mendel 12,13.
The most common clinical presentation is intermittent fever, unintentional weight loss, systemic or multiorgan abnormalities, and a personal previous history of any immunodeficiency. This is also described as a rare occurrence of disseminated intravascular coagulation 14. The earliest clinical signs include local erythema that evolves to a progressive edema in the ipsilateral axillary right region (the injection site). This can develop as purulent drainage, generalized lymphadenopathy, mucocutaneous rash, bone involvement, hepatosplenomegaly, and cough. The diagnosis criteria are the existence of systemic symptoms, such as fever, fatigue, weight loss, and malaise, and 2 or more involved areas. The definitive diagnostic criteria are the presence of a BCG vaccination scar with isolation of M. bovis. Therefore, culture and PCR, along with histopathological examination demonstrating granulomatous inflammation and M. bovis, are necessary 15,16.
Biểu hiện lâm sàng phổ biến nhất là sốt ngắt quãng, sụt cân ngoài ý muốn, các bất thường hệ thống hoặc đa cơ quan, và tiền sử cá nhân từng bị bất kỳ tình trạng suy giảm miễn dịch nào. Tình trạng này cũng được mô tả là một trường hợp hiếm gặp của đông máu rải rác trong lòng mạch 14. Các dấu hiệu lâm sàng sớm nhất bao gồm ban đỏ tại chỗ tiến triển thành phù nề tăng dần ở vùng nách bên phải cùng bên (vị trí tiêm). Tình trạng này có thể tiến triển thành rò mủ, bệnh hạch bạch huyết toàn thân, phát ban ở da niêm mạc, tổn thương xương, gan lách to và ho. Tiêu chuẩn chẩn đoán là sự hiện diện của các triệu chứng toàn thân, chẳng hạn như sốt, mệt mỏi, sụt cân, khó chịu và có từ 2 vùng trở lên bị ảnh hưởng. Tiêu chuẩn chẩn đoán xác định là sự hiện diện của sẹo tiêm vắc-xin BCG cùng với việc phân lập được M. bovis. Do đó, việc nuôi cấy và xét nghiệm PCR, cùng với xét nghiệm mô bệnh học chứng minh tình trạng viêm u hạt và sự hiện diện của M. bovis, là vô cùng cần thiết 15,16.
An important differential diagnosis is scrofuloderma due to M. bovis, which corresponded in the past to 10% of extrapulmonary TB. It usually presents with scrofuloderma, a direct extension of deeper infection to the cutaneous surface, lymphadenopathy, and phlogistic and infectious signs such as fever, mainly in patients with risk factors. To establish the diagnosis, it is necessary to identify M. bovis by PCR or culture. Before the implementation of food safety practices such as pasteurization, M. bovis was heavily associated with scrofula, but now accounts for less than 2% of TB infections in developed countries, such as the United States. Therefore, the pathophysiological mechanism is different, as scrofuloderma is a TB form and not a BCG-induced disease 17.
Một chẩn đoán phân biệt quan trọng là lao da cự lự (scrofuloderma) do M. bovis, bệnh lý mà trong quá khứ chiếm 10% các trường hợp lao ngoài phổi. Bệnh thường biểu hiện dưới dạng lao da cự lự, một sự lan rộng trực tiếp của nhiễm trùng sâu hơn lên bề mặt da, bệnh hạch bạch huyết, và các dấu hiệu viêm tấy cũng như nhiễm trùng như sốt, chủ yếu ở những bệnh nhân có các yếu tố nguy cơ. Để thiết lập chẩn đoán, cần phải định danh M. bovis bằng xét nghiệm PCR hoặc nuôi cấy. Trước khi áp dụng các biện pháp an toàn thực phẩm như tiêm trùng pasteur, M. bovis liên quan rất nhiều đến bệnh hạch cổ (scrofula), nhưng hiện nay chiếm chưa đến 2% các trường hợp nhiễm lao ở các nước phát triển, chẳng hạn như Hoa Kỳ. Do đó, cơ chế bệnh sinh là khác nhau, vì lao da cự lự là một dạng bệnh lao (TB) chứ không phải là bệnh do BCG gây ra 17.
Primary immunodeficiency diseases are inherited disorders of the immune system that increase the susceptibility to vaccination complications and infections. The most common type of immunodeficiency disorder is severe combined immunodeficiency syndrome, followed by unspecified immunodeficiency (nonspecific changes in CD3, CD4, and CD8 counts on peripheral blood flow cytometry) 17,18. Basic immune screening to determine underlying immune defects should include serum immunoglobulin levels (IgG, IgA, IgM, and IgE), lymphocyte subsets (CD3+, CD4+, CD8+ T cells; B cells, CD19+; and CD56+ natural killer cells), HIV serology, and neutrophil and interferon-gamma/interleukin-12 oxidation tests. In the present case, the results of these initial complementary tests were normal 19.
Các bệnh suy giảm miễn dịch bẩm sinh là những rối loạn di truyền của hệ miễn dịch làm tăng tính dễ bị tổn thương đối với các biến chứng tiêm chủng và nhiễm trùng. Loại rối loạn suy giảm miễn dịch phổ biến nhất là hội chứng suy giảm miễn dịch phối hợp nghiêm trọng, tiếp theo là suy giảm miễn dịch không đặc hiệu (các thay đổi không đặc hiệu về số lượng tế bào CD3, CD4 và CD8 trên xét nghiệm đếm tế bào dòng chảy máu ngoại vi) 17,18. Xét nghiệm tầm soát miễn dịch cơ bản để xác định các khiếm khuyết miễn dịch tiềm ẩn nên bao gồm nồng độ immunoglobulin huyết thanh (IgG, IgA, IgM và IgE), các phân nhóm lympho bào (tế bào T CD3+, CD4+, CD8+; tế bào B, CD19+; và tế bào giết tự nhiên CD56+), huyết thanh chẩn đoán HIV, và các xét nghiệm phản ứng oxy hóa của bạch cầu trung tính và interferon-gamma/interleukin-12. Trong ca bệnh này, kết quả của các xét nghiệm cận lâm sàng ban đầu này đều bình thường 19.
In addition, genetic analysis can help detect susceptibility to BCG disorders. The most commonly identified gene alleles in primary immunodeficiency diseases are IL7R, IL2RG, NHEJ1, CYBB, and IL12RB1, with X-linked recessive or autosomal recessive inheritance. Furthermore, additional c.306C and c.270-1G variants of IL2RG, c.87T of CYBB, and deletion of exons 10 and 11 of IL12RB1 have been more rarely reported previously 17,19. In previous patients, there are very few reports of BCGitis in adults, and most were in the non-disseminated form. Inoculation-site abscesses and erythematous nodules distant from the BCG injection site are exceedingly rare in the immunocompetent population. We did not find any cases of disseminated BCGitis in previous healthy children 20,21.
Ngoài ra, phân tích di truyền có thể giúp phát hiện tính dễ mắc các rối loạn do BCG. Các alen gen được xác định phổ biến nhất trong các bệnh suy giảm miễn dịch bẩm sinh là IL7R, IL2RG, NHEJ1, CYBB và IL12RB1, với kiểu di truyền lặn liên kết nhiễm sắc thể X hoặc lặn trên nhiễm sắc thể thường. Hơn nữa, các biến thể c.306C và c.270-1G bổ sung của IL2RG, c.87T của CYBB, và đột biến mất đoạn các exon 10 và 11 của IL12RB1 đã được báo cáo hiếm gặp hơn trước đây 17,19. Ở các bệnh nhân trước đây, có rất ít báo cáo về viêm hạch BCG ở người trưởng thành, và hầu hết đều ở dạng không lan tỏa. Áp-xe tại vị trí tiêm và các nốt ban đỏ ở xa vị trí tiêm BCG là cực kỳ hiếm gặp ở quần thể người có miễn dịch bình thường. Chúng tôi không tìm thấy bất kỳ trường hợp viêm hạch BCG lan tỏa nào ở trẻ em khỏe mạnh trước đây 20,21.
There is no consensus treatment strategy for disseminated BCGitis, either for medications or duration of treatment. Nevertheless, most reports, case series, and literature reviews report choosing to use the RIE regimen for 6 months. The regimen can be used alone or in combination with corticosteroids, and the infection usually resolves with no sequelae. The sensitivity to isoniazid and rifampicin are satisfied in general BCG vaccine strains currently in use 1–3,21. This double combination is usually effective and non-inferior, compared with other multidrug regimens containing more than 2 antitubercular drugs. The duration of therapy can vary from months to years, depending on the response and underlying immune defects. M. bovis is intrinsically resistant to pyrazinamide 21,22. Böhm et al and Cabas et al proposed more extensive studies and a systematic review on the treatment of disseminated BCGiitis. They recommend an anti-TB regimen with isoniazid, rifampicin, pyrazinamide, and ethambutol for 2 months and maintenance therapy with isoniazid and rifampicin for 6 months (rifampicin, isoniazid, and prednisone). Although their studies primarily evaluated BCGiitis after intravesical BCG injection for bladder tumors and in adult patients, we chose to follow their recommendation for our patient because they were the consensus, with the largest number of patients, results, and safety data that we found. Therefore, we used the RIE regimen, as pyrazinamide is not recommended in children, and we completed a total of 7 months of treatment. Throughout treatment, monitoring of clinical and laboratory inflammatory parameters is necessary, even after hospital discharge, as are support and monitoring of the patient’s nutritional and physical status 23,24.
Hiện chưa có chiến lược điều trị đồng thuận cho viêm hạch BCG lan tỏa, cả về thuốc sử dụng lẫn thời gian điều trị. Tuy nhiên, hầu hết các báo cáo, chuỗi ca bệnh và tổng quan tài liệu y văn đều ghi nhận việc lựa chọn sử dụng phác đồ RIE trong 6 tháng. Phác đồ này có thể được sử dụng đơn độc hoặc kết hợp với corticosteroid, và tình trạng nhiễm trùng thường thuyên giảm mà không để lại di chứng. Độ nhạy cảm với isoniazid và rifampicin được đáp ứng tốt ở các chủng vắc-xin BCG nói chung hiện đang được sử dụng 1–3,21. Sự kết hợp đôi này thường có hiệu quả và không kém hơn so với các phác đồ phối hợp nhiều thuốc khác chứa nhiều hơn 2 thuốc chống lao. Thời gian điều trị có thể thay đổi từ vài tháng đến vài năm, tùy thuộc vào đáp ứng và các khiếm khuyết miễn dịch tiềm ẩn. M. bovis có đặc tính kháng tự nhiên với pyrazinamide 21,22. Böhm và các cộng sự cùng với Cabas và các cộng sự đã đề xuất các nghiên cứu sâu rộng hơn và một tổng quan hệ thống về việc điều trị viêm hạch BCG lan tỏa. Họ khuyến cáo một phác đồ chống lao với isoniazid, rifampicin, pyrazinamide và ethambutol trong 2 tháng và liệu pháp duy trì với isoniazid và rifampicin trong 6 tháng (rifampicin, isoniazid và prednisone). Mặc dù các nghiên cứu của họ chủ yếu đánh giá tình trạng viêm hạch BCG sau khi bơm BCG vào bàng quang để điều trị u bàng quang và ở bệnh nhân trưởng thành, chúng tôi vẫn chọn làm theo khuyến cáo của họ cho bệnh nhân của mình vì đây là sự đồng thuận có số lượng bệnh nhân, kết quả và dữ liệu an toàn lớn nhất mà chúng tôi tìm thấy. Do đó, chúng tôi đã sử dụng phác đồ RIE, vì pyrazinamide không được khuyến cáo ở trẻ em, và chúng tôi đã hoàn thành tổng cộng 7 tháng điều trị. Trong suốt quá trình điều trị, việc theo dõi các chỉ số viêm trên lâm sàng và cận lâm sàng là cần thiết, ngay cả sau khi xuất viện, cũng như việc hỗ trợ và theo dõi tình trạng dinh dưỡng và thể chất của bệnh nhân 23,24.
Moxifloxacin might be considered for about 10 months in children with BCGitis 25. There are many reported cases with intravenous antibiotics, antivirals, and antifungals associated with antitubercular treatment, especially when the diagnosis was not fulfilled or was delayed 26,27. Our patient was treated for 7 months with RIE, and we stopped only after complete resolution. We considered that the possible adverse effects of ethambutol (mainly impaired vision) were outweighed by the severity of this case. Isoniazid is metabolized in the liver, leading to hepatotoxic metabolites of hydrazine and acetyl hydrazine, with an incidence of 0.6% of hepatotoxicity, hepatocellular necrosis, and steatosis. Rifampicin can cause cholestasis, elevation of conjugated bilirubin, and transient transaminitis, which is often benign. Rarely, it is associated with centrilobular parenchymal necrosis 28,29.
Moxifloxacin có thể được cân nhắc sử dụng trong khoảng 10 tháng ở trẻ em bị viêm hạch BCG 25. Có nhiều trường hợp được báo cáo đã sử dụng kháng sinh, thuốc kháng virus và thuốc kháng nấm đường tĩnh mạch kết hợp với điều trị chống lao, đặc biệt là khi chẩn đoán chưa được xác định hoặc bị trì hoãn 26,27. Bệnh nhân của chúng tôi đã được điều trị trong 7 tháng với RIE, và chúng tôi chỉ ngừng thuốc sau khi bệnh thuyên giảm hoàn toàn. Chúng tôi nhận thấy rằng các tác dụng bất lợi có thể xảy ra của ethambutol (chủ yếu là suy giảm thị lực) đã được bù đắp thỏa đáng bởi mức độ nghiêm trọng của ca bệnh này. Isoniazid được chuyển hóa ở gan, tạo ra các chất chuyển hóa độc cho gan là hydrazine và acetyl hydrazine, với tỷ lệ độc tính trên gan là 0,6%, gây hoại tử tế bào gan và thoái hóa mỡ. Rifampicin có thể gây ứ mật, tăng bilirubin liên hợp và tăng men gan thoáng qua, tình trạng này thường lành tính. Hiếm khi nó liên quan đến hoại tử nhu mô trung tâm tiểu thùy 28,29.
A replacement dose of intravenous immunoglobulin is also important when specific immunosuppression is detected. Alternative vaccinations can be considered when immunosuppressants are previously known or in siblings of patients who had disseminated BCGitis, and include antigen-based vaccines, Mycobacterium tuberculosis (MTB) vaccines, recombinant BCG vaccines, and attenuated MTB vaccines 30,31.
Việc sử dụng liều thay thế immunoglobulin truyền tĩnh mạch cũng quan trọng khi phát hiện tình trạng suy giảm miễn dịch đặc hiệu. Các giải pháp vắc-xin thay thế có thể được cân nhắc khi tình trạng suy giảm miễn dịch đã được biết trước hoặc ở anh chị em ruột của những bệnh nhân từng bị viêm hạch BCG lan tỏa, bao gồm vắc-xin dựa trên kháng nguyên, vắc-xin kháng Mycobacterium tuberculosis (MTB), vắc-xin BCG tái tổ hợp và vắc-xin MTB giảm độc lực 30,31.
Conclusions
Kết luận
We report an unusually severe course of M. bovis vaccine-associated disease in a previously healthy infant with negative screening for primary immunodeficiency who achieved full recovery with RIE therapy, without sequelae. Clinicians should remain vigilant for disseminated BCGitis, even in immunocompetent patients. Further studies are needed to refine diagnostic and treatment strategies; however, the RIE regimen used in this case was highly effective.
Chúng tôi báo cáo một diễn tiến nặng nề bất thường của bệnh lý liên quan đến vắc-xin M. bovis ở một trẻ sơ sinh trước đó khỏe mạnh, có kết quả tầm soát âm tính với tình trạng suy giảm miễn dịch bẩm sinh, trẻ đã đạt được sự hồi phục hoàn toàn nhờ liệu pháp RIE và không để lại di chứng. Các bác sĩ lâm sàng cần duy trì sự cảnh giác đối với tình trạng viêm hạch BCG lan tỏa, ngay cả ở những bệnh nhân có miễn dịch bình thường. Cần có thêm các nghiên cứu để hoàn thiện các chiến lược chẩn đoán và điều trị; tuy nhiên, phác đồ RIE được sử dụng trong ca bệnh này đã mang lại hiệu quả rất cao.
Reference
- Lyra PT, Souza E, Moura ACA, Inborn errors of immunity in patients with adverse events following BCG vaccination in Brazil: J Clin Immunol, 2022; 42(8); 1708-20
- Soyak Aytekin E, Keskin A, Tan C, Differential diagnosis of primary immunodeficiency in patients with BCGitis and BCGosis: A single-centre study: Scand J Immunol, 2021; 94(4); e13084
- Fekrvand S, Yazdani R, Olbrich P, Primary immunodeficiency diseases and Bacillus Calmette-Guérin (BCG)-vaccine-derived complications: A systematic review: J Allergy Clin Immunol Pract, 2020; 8(4); 1371-86
- Sellami K, Amouri M, Kmiha S, Adverse reactions due to the Bacillus Calmette-Guerin vaccine: Twenty Tunisian cases: Indian J Dermatol, 2018; 63(1); 62-65
- NaserEddin A, Dinur-Schejter Y, Shadur B, Bacillus Calmette-Guerin (BCG) vaccine-associated complications in immunodeficient patients following stem cell transplantation: J Clin Immunol, 2021; 41(1); 147-62
- Schembri Higgans J, Pace K, Systemic BCGosis following intra-renal instillation of BCG: A case report: J Surg Case Rep, 2021; 2021(12); rjab544
- Hesseling AC, Rabie H, Marais BJ, Bacille Calmette-Guérin vaccine-induced disease in HIV-infected and HIV-uninfected children: Clin Infect Dis, 2006; 42(4); 548-58
- Vallilas C, Zachou M, Dolkiras P, Difficulties in diagnosing and treating disseminated Bacillus Calmette-Guérin (BCG) infection After intravesical BCG therapy in a patient with liver cirrhosis: A case report: Am J Case Rep, 2021; 22; e933006
- Liu G, Xiao H, Liu L, Severe cases of BCGosis-susceptible primary immunodeficiency diseases identified by next-generation sequencing: Implications for adjustment of BCG vaccination timing in China: J Genet Genomics, 2020; 47(4); 229-32
- Andrade de Souza R, Rodrigues Barreto F, Antônio de Souza Teles Santos C, Evolution of the Bacillus Calmette-Guérin scar Russia and Moreau strains in newborns: A Brazilian cohort: Vaccine X, 2023; 14; 100323
- Diniz LM, Guimarães T, Rodrigues de Oliveira MdG: J Bras Pneumol, 2014; 40(2); 188-92
- Sohani M, Habibi S, Delavari S, Evaluation of patients with primary immunodeficiency associated with Bacille Calmette-Guerin (BCG)-vaccine-derived complications: Allergol Immunopathol (Madr), 2020; 48(6); 729-37
- Ladeira I, Carvalho I, Correia A, BCGitis in children: Rev Port Pneumol, 2014; 20(3); 172-73 [Erratum in: Rev Port Pneumol (2006). 2016;22(6):e1]
- Bukhari E, Alaklobi F, Bakheet H, Disseminated bacille Calmette-Guérin disease in Saudi children: Clinical profile, microbiology, immunology evaluation and outcome: Eur Rev Med Pharmacol Sci, 2016; 20(17); 3696-702
- Amanati A, Pouladfar G, Kadivar MR, A 25-year surveillance of disseminated Bacillus Calmette-Guérin disease treatment in children in Southern Iran: Medicine (Baltimore), 2017; 96(52); e9035
- Barkai G, Somech R, Stauber T, Bacille Calmette-Guerin (BCG) complications in children with severe combined immunodeficiency (SCID): Infect Dis (Lond), 2019; 51(8); 585-92
- Estrada VB, Lemos ACL, Luz PM, Scrofuloderma of the chest with mediastinal TB: Pediatr Dermatol, 2024; 41(5); 874-77
- Hassanzad M, Valinejadi A, Darougar S, Disseminated Bacille Calmette-Guérin infection at a glance: A mini review of the literature: Adv Respir Med, 2019; 87(4); 239-42
- Ong RYL, Chan SB, Chew SJ, Disseminated Bacillus-Calmette-Guérin infections and primary immunodeficiency disorders in singapore: A single center 15-year retrospective review: Int J Infect Dis, 2020; 97; 117-25
- Ozsezen B, Yalçýn E, Ademhan Tural D, Antimycobacterial prophylaxis regarding Bacillus Calmette-Guérin-associated complications in children with primary immunodeficiency: Respir Med, 2022; 200; 106919
- Elsidig N, Alshahrani D, Alshehri M, Bacillus Calmette-Guérin vaccine related lymphadenitis in children: Management guidelines endorsed by the Saudi Pediatric Infectious Diseases Society (SPIDS): Int J Pediatr Adolesc Med, 2015; 2(2); 89-95
- Abdalla A, Elbakri AS, Almatrooshi CA, Unexpected deltoid abscess from BCG Vaccination in a healthy adult: A case report: Am J Case Rep, 2025; 26; e946723
- Böhm WU, Koch R, Wenzel SDevelopment and treatment of localized/systemic BCGitis: Retrospective studies in direct comparison to mitomycin C: Urologe A, 2018; 57(5); 568-76 [in German]
- Cabas P, Rizzo M, Giuffrè M, BCG infection (BCGitis) following intravesical instillation for bladder cancer and time interval between treatment and presentation: A systematic review: Urol Oncol, 2021; 39(2); 85-92
- Alsuhaibani M, Felimban G, Shoukri M, Safety and tolerability of moxifloxacin for the treatment of disseminated BCGitis in children: Int J Pediatr Adolesc Med, 2019; 6(2); 47-50
- Keijsers RR, Bovenschen HJ, Seyger MM, Cutaneous complication after BCG vaccination: Case report and review of the literature: J Dermatolog Treat, 2011; 22(6); 315-18
- Lupon E, Martin-Blondel G, Pollon T, BCGitis of the wrist after intravesical BCG therapy: A case report: Hand Surg Rehabil, 2020; 39(6); 585-87
- Roduit A, Pouget R, Defabiani N, Troillet NBCGitis following intravesical administration of bacillus Calmette-Guérin: Rev Med Suisse, 2020; 16(710); 1920-23 [in French]
- Rajabi A, Pouladfar G, Dehghan Y, Disseminated Bacillus Calmette-Guérin infection: Role of imaging in the evaluation of complications: J Trop Pediatr, 2023; 69(4); fmad024
- Sharma S, Tanigasalam V, Parameswaran N, Fulminant BCG disease in a 7 month old healthy male infant: J Trop Pediatr, 2015; 61(6); 474-77
- Chitamanni P, Anbazhagan J, Parameswaran N, Vijayakumar S, BCGosis in infants with Severe Combined ImmunoDeficiency (SCID): Indian J Pediatr, 2018; 85(7); 585-86
Có thể bạn quan tâm
-
Đáp ứng với hormone tăng trưởng ở trẻ có đột biến TOMM7 đồng hợp tử: Những góc nhìn điều trị mới
Growth Hormone Response in a Child With a Homozygous TOMM7 Mutation: Novel Therapeutic Insights
-
Phẫu thuật nội soi so với phẫu thuật mở trong điều trị thoát vị bẹn ở trẻ em
Laparoscopic versus open repair for pediatric inguinal hernia
-
Việc tái phân loại cần sa mở ra cánh cửa cho nghiên cứu y học rất cần thiết về lợi ích và rủi ro của loại thuốc này
Reclassification of marijuana opens doors for much-needed medical research into the benefits and risks of the drug