Miễn phí
Hội chứng chèn ép khoang thứ phát sau viêm tắc tĩnh mạch xanh đau ở bệnh nhân mắc bệnh Crohn
Compartment Syndrome Secondary to Phlegmasia Cerulea Dolens in a Patient With Crohn’s Disease
Saad Mohammed Alshahrani; Raghad Ibrahim Alkoblan; Reem Abdulaziz Alturki; Shahad Mohammed Alashgar. American Journal of Case Reports. doi: 10.12659/AJCR.948950. Open access.

Figure 1
https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e948950-g001.jpg&idArt=948950&w=1000
Figure 1
Hình 1
Right lower limb swelling and blue discoloration.
Tình trạng sưng nề và đổi sang màu xanh ở chi dưới bên phải.
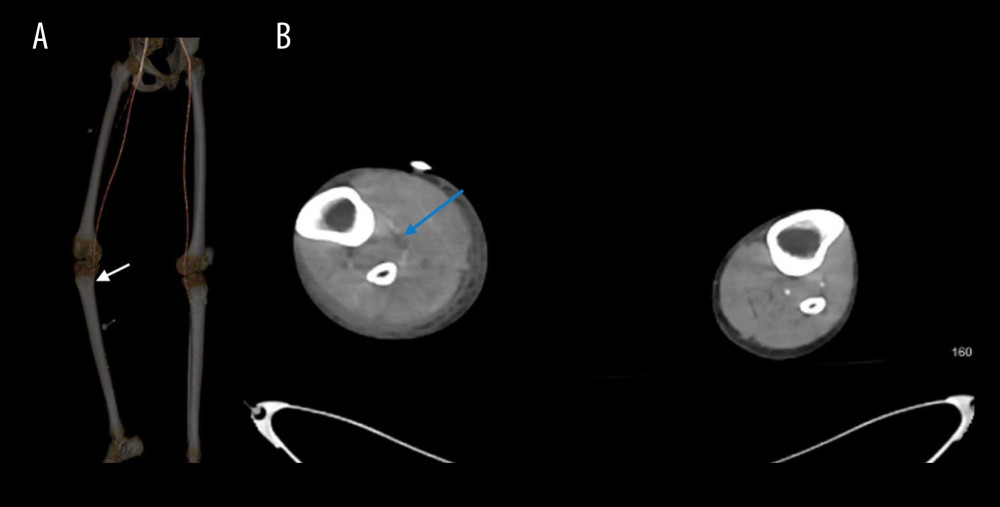
Figure 2
https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e948950-g002.jpg&idArt=948950&w=1000
Figure 2
Hình 2
Computed tomography imaging demonstrating progressive non-opacification of the right infrageniculate arteries. (A) Lower limb computed tomography angiography revealing progressive non-opacification of the right infrageniculate arteries with distal loss of opacification (white arrow). (B) Abdominopelvic computed tomography (cross-sectional view) showing progressive non-opacification of the right infrageniculate arteries (blue arrow).
Hình ảnh chụp cắt lớp vi tính cho thấy tình trạng không ngấm thuốc tiến triển của các động mạch dưới gối phải. (A) Chụp cắt lớp vi tính mạch máu chi dưới cho thấy tình trạng không ngấm thuốc tiến triển của các động mạch dưới gối phải kèm theo mất ngấm thuốc ở đoạn xa (mũi tên trắng). (B) Chụp cắt lớp vi tính bụng chậu (mặt cắt ngang) cho thấy tình trạng không ngấm thuốc tiến triển của các động mạch dưới gối phải (mũi tên xanh dương).
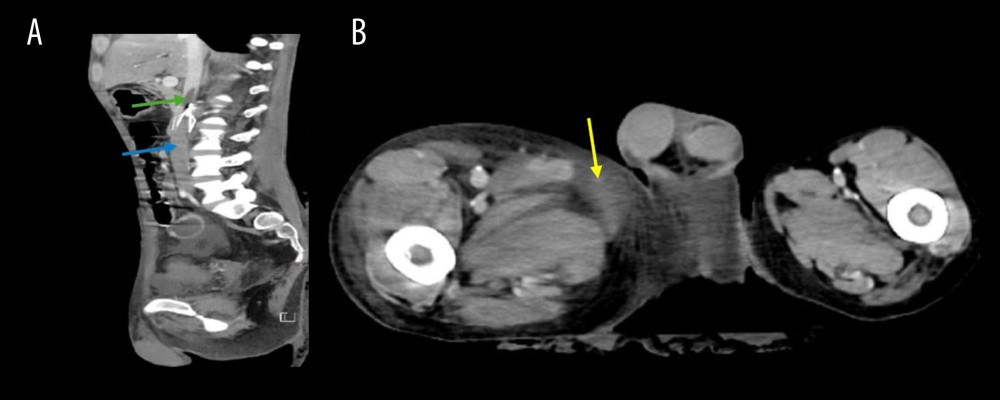
Figure 3
https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e948950-g003.jpg&idArt=948950&w=1000
Figure 3
Hình 3
Abdominopelvic computed tomography imaging demonstrating venous thrombosis and associated soft tissue changes. (A) Abdominopelvic computed tomography (sagittal view) showing venous thrombosis extending above the inferior vena cava (IVC) filter (green arrow) into the infrahepatic segment (blue arrow). The IVC filter is visible immediately below the green arrow but not separately labeled. (B) Abdominopelvic computed tomography (cross-sectional view) showing asymmetrical soft tissue enlargement and congestion in the right thigh (yellow arrow).
Hình ảnh chụp cắt lớp vi tính bụng chậu cho thấy huyết khối tĩnh mạch và các thay đổi mô mềm kèm theo. (A) Chụp cắt lớp vi tính bụng chậu (mặt cắt đứng dọc) cho thấy huyết khối tĩnh mạch lan rộng lên trên lưới lọc tĩnh mạch chủ dưới (IVC) (mũi tên xanh lá) đi vào đoạn dưới gan (mũi tên xanh dương). Lưới lọc IVC có thể nhìn thấy ngay phía dưới mũi tên xanh lá nhưng không được dán nhãn riêng biệt. (B) Chụp cắt lớp vi tính bụng chậu (mặt cắt ngang) cho thấy tình trạng sưng phồng mô mềm không đối xứng và sung huyết ở đùi phải (mũi tên vàng).
Có thể bạn quan tâm
-
Viêm cơ hoại tử do trung gian MDA5 liên quan đến COVID-19
COVID-19-Associated MDA5-Mediated Necrotizing Myositis
-
Các can thiệp dinh dưỡng qua đường miệng ở người cao tuổi nhập viện có nguy cơ suy dinh dưỡng: phân tích gộp mạng lưới dữ liệu từ từng người tham gia
Oral nutritional interventions in hospitalised older people at nutritional risk: a network meta-analysis of individual participant data
-
Rào cản đối với một sở thích: Biến đổi khí hậu và văn hóa ‘runfluencer’ tác động đến buổi chạy bộ hàng ngày của chúng ta
Hurdles to a hobby: How climate change and ‘runfluencer’ culture impact our daily jog