Miễn phí
Loại bỏ dị vật giác mạc bằng nhựa ở trẻ nhũ nhi 2 tháng tuổi: Báo cáo ca lâm sàng
Plastic Corneal Foreign Body Removal From a 2-Month-Old Infant: A Case Report
Shichun Chen; Ning Zhang; Huangpei Xu; Zhichao Cai; Liangwen Li; Suqian Wu. American Journal of Case Reports. doi: 10.12659/AJCR.950663. Open access.
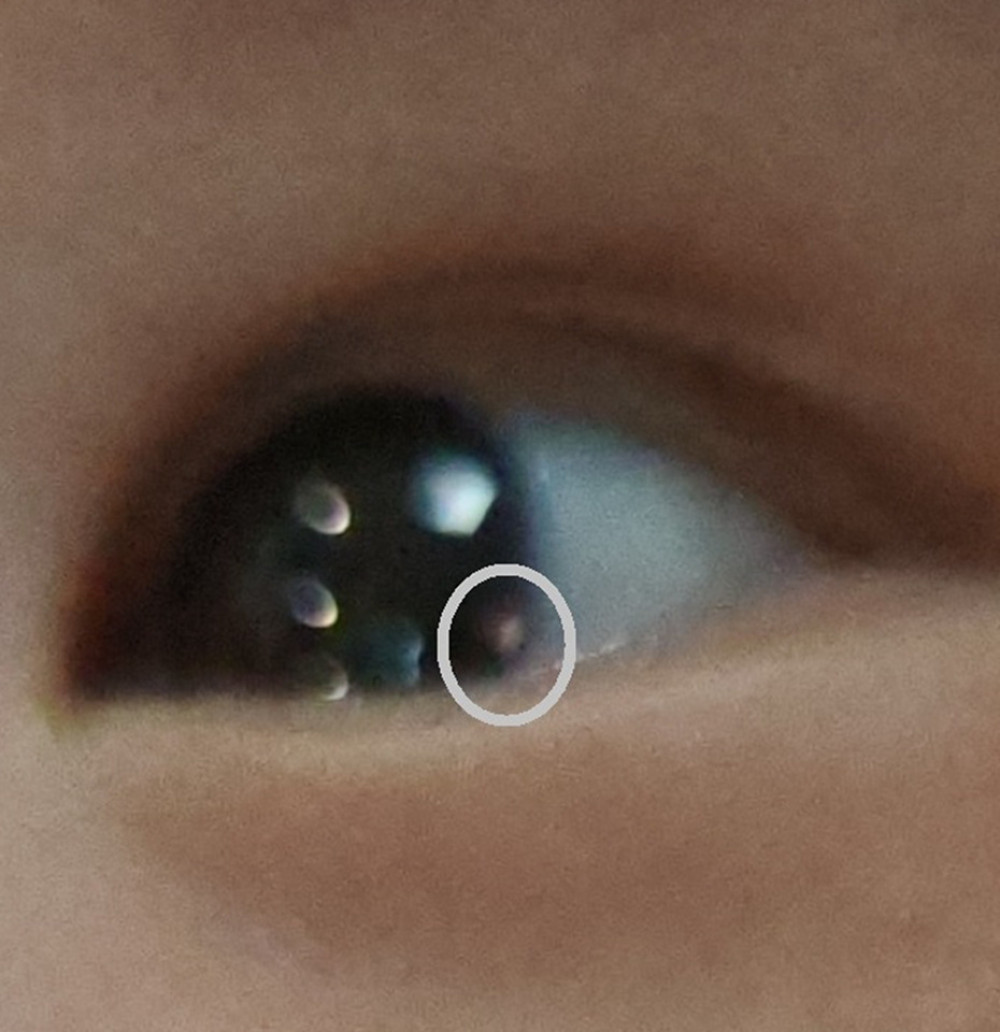
Figure 1
https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e950663-g001.jpg&idArt=950663&w=1000
Figure 1
Hình 1
Photo caption of a corneal foreign body (CFB) in the 2-month-old male. The white solid circle outlines an oval, pink plastic CFB located on the corneal surface, close to the inferior temporal limbus, with a diameter of approximately 0.8 mm.
Chú thích ảnh về dị vật giác mạc (CFB) ở bé trai 2 tháng tuổi. Vòng tròn trắng nét liền khoanh vùng một dị vật giác mạc bằng nhựa màu hồng, hình bầu dục nằm trên bề mặt giác mạc, sát vùng rìa phía dưới – thái dương, với đường kính khoảng 0.8 mm.
Có thể bạn quan tâm
-
Đặc điểm của các tổn thương giả cành cây ở giác mạc trong bệnh tăng tyrosine máu bẩm sinh tuýp 1 trên kính hiển vi đồng tiêu trong cơ thể và chụp cắt lớp quang học bán phần trước
In Vivo Confocal Microscopy and Anterior Segment Optical Coherence Tomography Features of Corneal Pseudodendritic Lesions in Hereditary Tyrosinemia Type 1
-
Cố định lưới xuyên mô so với cố định lưới không xuyên mô trong phẫu thuật nội soi điều trị thoát vị bẹn
Penetrating versus non-penetrating mesh fixation in laparoscopic groin hernia repair
-
Dị ứng phấn hoa năm nay rất nặng – bác sĩ giải thích lý do, và cách tìm cách giảm nhẹ
Pollen allergies are brutal this year – a doctor explains why, and how to find relief