Ca lâm sàng
Viêm mạch u hạt tăng bạch cầu ái toan âm tính với ANCA biểu hiện bằng hẹp tá tràng: Một báo cáo ca lâm sàng
ANCA-Negative Eosinophilic Granulomatosis With Polyangiitis Presenting With Duodenal Stenosis: A Case Report
Abstract
Tóm tắt
BACKGROUND: Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare ANCA-associated vasculitis characterized by asthma, eosinophilia, and multi-organ involvement. Duodenal stenosis is an uncommon gastrointestinal complication, with few reported cases linked to EGPA.
BỐI CẢNH: Viêm mạch u hạt tăng bạch cầu ái toan (EGPA) là một bệnh viêm mạch hiếm gặp liên quan đến ANCA, đặc trưng bởi hen suyễn, tăng bạch cầu ái toan và tổn thương đa cơ quan. Hẹp tá tràng là một biến chứng tiêu hóa ít gặp, với rất ít trường hợp được báo cáo có liên quan đến EGPA.
CASE REPORT: A 71-year-old man with a 2-week history of recurrent abdominal distension and pain was admitted to our hospital. Notably, there was a marked elevation in absolute eosinophil count (1.13×10⁹/L) and eosinophils (14.3%), while ANCA was negative. Additionally, elevated levels of erythrocyte sedimentation rate and C-reactive protein were observed. Electronic gastroscopy revealed duodenal bulb stenosis, with pathological findings indicating significant eosinophil infiltration. The patient, with a history of asthma, exhibited neurological impairment symptoms alongside elevated eosinophil levels. After excluding parasitic infections, hypereosinophilic syndrome, and eosinophilic gastroenteritis based on systemic involvement and diagnostic criteria, EGPA was considered as the diagnosis. Following treatment with methylprednisolone (0.8 mg/kg/day) and cyclophosphamide (5 mg/kg IV every 2 weeks), the patient experienced substantial relief in abdominal distension and pain symptoms. Concurrently, parameters including eosinophil count, C-reactive protein level, and erythrocyte sedimentation rate progressively normalized. The 4-month follow-up gastroscopy showed significant improvement of duodenal stenosis.
BÁO CÁO CA LÂM SÀNG: Một nam bệnh nhân 71 tuổi có tiền sử 2 tuần bị đau và chướng bụng tái phát đã nhập viện chúng tôi. Đáng chú ý, có sự gia tăng rõ rệt về số lượng bạch cầu ái toan tuyệt đối (1.13×10⁹/L) và tỷ lệ bạch cầu ái toan (14.3%), trong khi ANCA âm tính. Thêm vào đó, nồng độ protein phản ứng C và tốc độ lắng máu cũng tăng cao. Nội soi dạ dày ống mềm phát hiện hẹp hành tá tràng, với kết quả giải phẫu bệnh cho thấy sự thâm nhiễm bạch cầu ái toan đáng kể. Bệnh nhân có tiền sử hen suyễn, biểu hiện các triệu chứng suy giảm thần kinh đi kèm với nồng độ bạch cầu ái toan tăng cao. Sau khi loại trừ nhiễm ký sinh trùng, hội chứng tăng bạch cầu ái toan và viêm dạ dày ruột tăng bạch cầu ái toan dựa trên tổn thương hệ thống và các tiêu chuẩn chẩn đoán, EGPA đã được xem xét để chẩn đoán. Sau khi điều trị bằng methylprednisolone (0.8 mg/kg/ngày) và cyclophosphamide (5 mg/kg truyền tĩnh mạch mỗi 2 tuần), bệnh nhân đã thuyên giảm đáng kể các triệu chứng đau và chướng bụng. Đồng thời, các chỉ số bao gồm số lượng bạch cầu ái toan, nồng độ protein phản ứng C và tốc độ lắng máu dần trở lại bình thường. Nội soi dạ dày theo dõi sau 4 tháng cho thấy tình trạng hẹp tá tràng đã cải thiện rõ rệt.
CONCLUSIONS: Duodenal stenosis is a rare but serious manifestation of EGPA, likely resulting from eosinophilic infiltration and inflammation. This case highlights the need to consider EGPA in asthmatic patients presenting with gastrointestinal obstruction and eosinophilia. Early immunosuppressive therapy can improve outcomes, and endoscopic evaluation remains essential. Even without classic vasculitic histology, EGPA can be diagnosed based on systemic criteria, with gastrointestinal obstruction as a potential initial manifestation.
KẾT LUẬN: Hẹp tá tràng là một biểu hiện hiếm gặp nhưng nghiêm trọng của EGPA, có khả năng là kết quả của tình trạng viêm và thâm nhiễm bạch cầu ái toan. Ca lâm sàng này nhấn mạnh nhu cầu cần xem xét chẩn đoán EGPA ở những bệnh nhân hen suyễn có biểu hiện tắc nghẽn tiêu hóa và tăng bạch cầu ái toan. Liệu pháp ức chế miễn dịch sớm có thể cải thiện kết quả điều trị, và việc đánh giá qua nội soi vẫn đóng vai trò thiết yếu. Ngay cả khi không có hình ảnh mô bệnh học viêm mạch điển hình, EGPA vẫn có thể được chẩn đoán dựa trên các tiêu chuẩn hệ thống, với tắc nghẽn tiêu hóa là một biểu hiện ban đầu tiềm tàng.
Keywords: duodenum, vasculitis, eosinophilia
Từ khóa: Tá tràng, Viêm mạch, Tăng bạch cầu ái toan
Introduction
Đặt vấn đề
Eosinophilic granulomatosis with polyangiitis (EGPA), previously referred to as Churg-Strauss syndrome, is an antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis primarily affecting small- to medium-sized blood vessels. It is pathologically characterized by eosinophil-rich tissue infiltration, necrotizing vasculitis, and granulomatous inflammation. Unlike the other 2 types of ANCA-associated vasculitis (granulomatosis with polyangiitis and microscopic polyangiitis), EGPA is characterized by asthma, sinusitis, eosinophilia, and eosinophil infiltration in tissues and blood 1. Gastrointestinal involvement is reported in approximately 20% to 30% of patients with EGPA and is associated with significant morbidity and a poorer prognosis 2. Duodenal stenosis is frequently attributed to ulcers, Crohn disease, and tumors. However, when associated with eosinophilia, eosinophilic gastroenteritis (EGID) is the most common cause. Duodenal stenosis as a direct manifestation of EGPA is exceptionally rare, with limited documentation on the combination of EGPA and duodenal stenosis. In this case report, we describe a unique presentation of ANCA-negative EGPA manifesting as duodenal stenosis, underscoring the diagnostic challenges and the importance of a multidisciplinary approach.
Viêm mạch u hạt tăng bạch cầu ái toan (EGPA), trước đây gọi là hội chứng Churg-Strauss, là một bệnh viêm mạch liên quan đến kháng thể kháng bào tương bạch cầu đa nhân trung tính (ANCA), chủ yếu ảnh hưởng đến các mạch máu kích thước nhỏ đến trung bình. Về mặt bệnh học, bệnh đặc trưng bởi tình trạng thâm nhiễm mô giàu bạch cầu ái toan, viêm mạch hoại tử và viêm u hạt. Không giống như 2 loại viêm mạch liên quan đến ANCA khác (viêm mạch u hạt và viêm vi mạch hệ thống), EGPA đặc trưng bởi hen suyễn, viêm xoang, tăng bạch cầu ái toan, và thâm nhiễm bạch cầu ái toan trong mô và máu 1. Tổn thương đường tiêu hóa được báo cáo ở khoảng 20% đến 30% bệnh nhân mắc EGPA và có liên quan đến tỷ lệ mắc bệnh cao cùng tiên lượng xấu hơn 2. Hẹp tá tràng thường do loét, bệnh Crohn và các khối u. Tuy nhiên, khi đi kèm với tình trạng tăng bạch cầu ái toan, viêm dạ dày ruột tăng bạch cầu ái toan (EGID) là nguyên nhân phổ biến nhất. Hẹp tá tràng như một biểu hiện trực tiếp của EGPA là cực kỳ hiếm gặp, với các tài liệu ghi nhận còn hạn chế về sự kết hợp giữa EGPA và hẹp tá tràng. Trong báo cáo ca lâm sàng này, chúng tôi mô tả một bệnh cảnh độc đáo của EGPA âm tính với ANCA biểu hiện dưới dạng hẹp tá tràng, qua đó nhấn mạnh những thách thức trong chẩn đoán và tầm quan trọng của phương pháp tiếp cận đa chuyên khoa.
Case Report
Báo cáo ca lâm sàng
Additional diagnostic workup
Các xét nghiệm chẩn đoán bổ sung
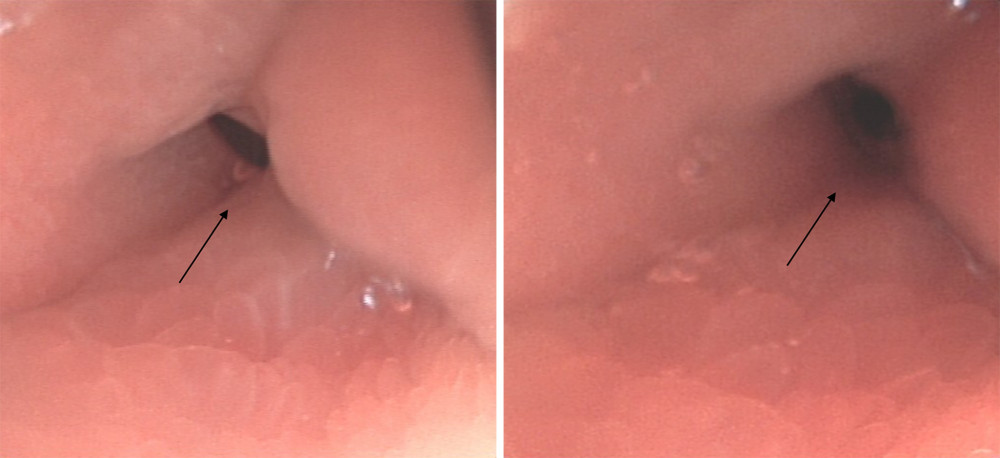
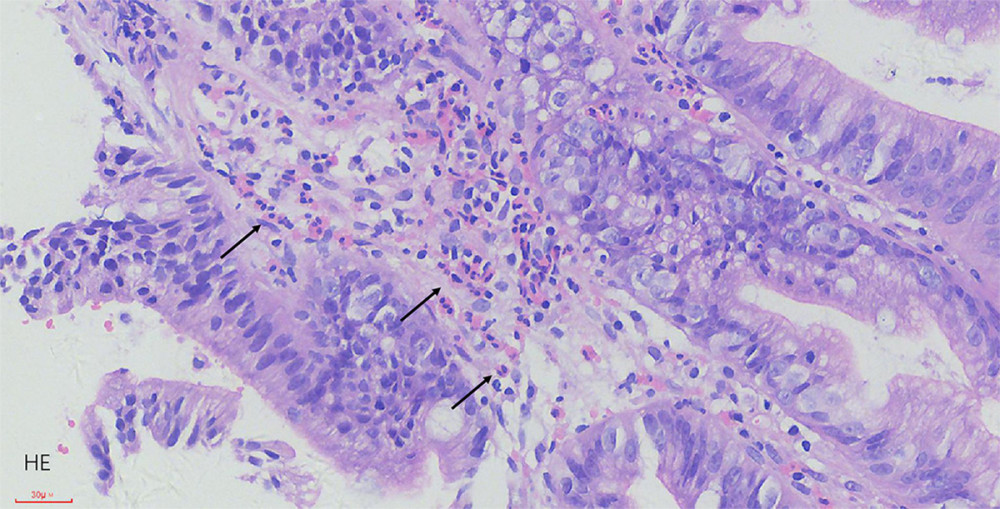
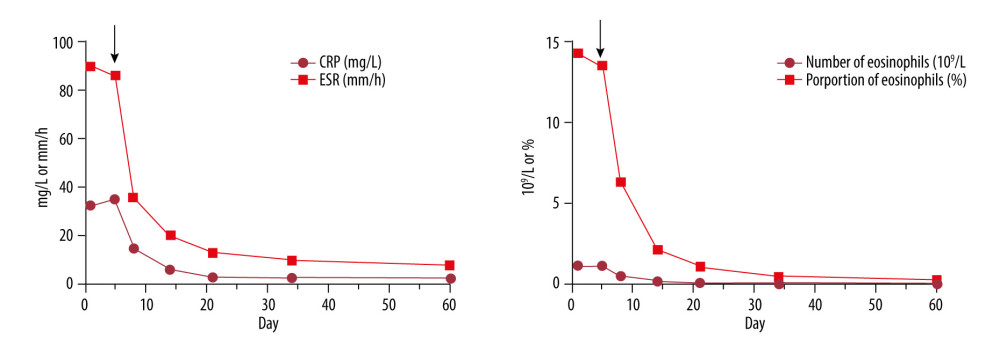
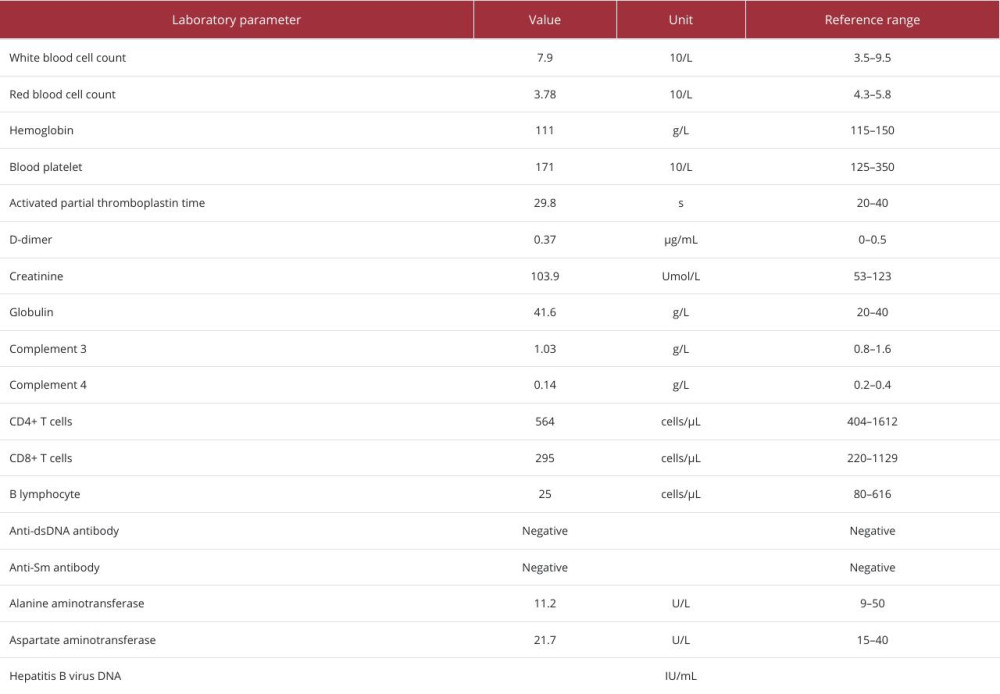
Endoscopic examination revealed deformation and edema in the duodenal bulb, accompanied by stenosis at the junction of the duodenal bulb and its descending portion (Figure 1). Pathological examination of the duodenal bulb indicated extensive eosinophil infiltration (>20 eosinophils per high-power field in the mucosal layer; Figure 2). The biopsy was limited to the mucosa and submucosa; no vasculitis or granulomas were identified in the sampled tissue. Bilateral pure tone audiometry indicated sensorineural hearing loss (primarily in the high frequencies, mild to moderate in degree), with normal middle ear transmission function. A chest computed tomography (CT) scan showed emphysema accompanied by local nodular thickening of the pleura. A sinus CT scan revealed mild mucosal thickening in the maxillary sinuses. Nerve conduction studies and fundus examination were offered, but the patient declined. Laboratory test results indicated an increase in the proportion of eosinophils (14.3%) and absolute eosinophil count (1.13×109/L), as well as increased levels of erythrocyte sedimentation rate (ESR, 90 mm/h), C-reactive protein (CRP, 32.5 mg/L), and ANA titer (1: 100). Laboratory investigations revealed an elevated total IgE level of 450 IU/mL. Stool examination for ova and parasites was negative, and serological tests for common parasites (eg, Strongyloides) were also negative. Urinalysis showed no proteinuria or active sediment. The serum creatinine level was within the reference range. Cardiac evaluation included a normal troponin I level, NT-proBNP level, and echocardiogram. Both the cytoplasmic ANCA and perinuclear ANCA tests were negative. The remaining laboratory test results and the dynamic changes in ESR, CRP, and eosinophil counts are presented in Table 1 and Figure 3. On admission, vital signs were as follows: blood pressure of 128/73 mmHg, pulse rate of 82 beats/min, respiratory rate of 18 breaths/min, and body temperature of 36.7°C. Physical examination revealed mild tenderness in the upper abdomen and decreased breath sounds in both lungs.
Nội soi cho thấy biến dạng và phù nề ở hành tá tràng, kèm theo hẹp tại vị trí nối giữa hành tá tràng và phần xuống của tá tràng (Figure 1). Kết quả giải phẫu bệnh của hành tá tràng cho thấy sự thâm nhiễm bạch cầu ái toan lan rộng (>20 bạch cầu ái toan trên mỗi vi trường độ phóng đại lớn ở lớp niêm mạc; Figure 2). Sinh thiết chỉ giới hạn ở lớp niêm mạc và dưới niêm mạc; không phát hiện tình trạng viêm mạch hoặc u hạt trong mô được lấy mẫu. Đo thính lực đồ âm chuẩn hai bên cho thấy mất thính lực tiếp nhận (chủ yếu ở tần số cao, mức độ nhẹ đến trung bình), với chức năng truyền âm tai giữa bình thường. Chụp cắt lớp vi tính (CT) ngực cho thấy tình trạng khí phế thũng kèm theo dày nốt cục bộ màng phổi. Chụp CT xoang cho thấy niêm mạc xoang hàm dày nhẹ. Bệnh nhân được đề nghị thực hiện các xét nghiệm dẫn truyền thần kinh và khám đáy mắt nhưng đã từ chối. Kết quả xét nghiệm cho thấy tỷ lệ bạch cầu ái toan tăng (14.3%) và số lượng bạch cầu ái toan tuyệt đối tăng (1.13×109/L), cũng như mức độ tăng của tốc độ lắng máu (ESR, 90 mm/h), protein phản ứng C (CRP, 32.5 mg/L) và hiệu giá ANA (1: 100). Các xét nghiệm cận lâm sàng cho thấy nồng độ IgE toàn phần tăng lên 450 IU/mL. Xét nghiệm phân tìm ký sinh trùng và trứng giun sán âm tính, các xét nghiệm huyết thanh học với các loại ký sinh trùng phổ biến (ví dụ: Strongyloides) cũng âm tính. Tổng phân tích nước tiểu không thấy protein niệu hoặc cặn lắng hoạt động. Nồng độ creatinine huyết thanh nằm trong ngưỡng tham chiếu. Đánh giá tim mạch bao gồm mức troponin I, NT-proBNP và siêu âm tim đều bình thường. Cả hai xét nghiệm ANCA bào tương và ANCA quanh nhân đều âm tính. Các kết quả xét nghiệm còn lại và những thay đổi động học của ESR, CRP và số lượng bạch cầu ái toan được trình bày trong Table 1 và Figure 3. Khi nhập viện, các dấu hiệu sinh tồn như sau: huyết áp 128/73 mmHg, nhịp mạch 82 lần/phút, nhịp thở 18 lần/phút và thân nhiệt 36.7°C. Khám thực thể cho thấy bụng trên ấn đau nhẹ và rì rào phế nang giảm ở cả hai phổi.
Differential diagnosis
Chẩn đoán phân biệt
The differential diagnosis for eosinophilia with gastrointestinal obstruction included parasitic infection, hypereosinophilic syndrome (HES), and EGID. The absence of travel history, negative stool and serology tests, and the presence of systemic features (asthma, sinusitis, neuropathy) provided evidence against parasitic infection. The lack of a clonal hematopoietic disorder and the presence of asthma and vasculitic features (although not histologically confirmed) made HES less likely. While EGID can cause transmural eosinophilic infiltration and stenosis, the combination with extra-intestinal manifestations such as neuropathy and a long-standing history of asthma strongly favored the diagnosis of EGPA.
Chẩn đoán phân biệt cho tình trạng tăng bạch cầu ái toan kèm tắc nghẽn đường tiêu hóa bao gồm nhiễm ký sinh trùng, hội chứng tăng bạch cầu ái toan (HES) và viêm dạ dày ruột tăng bạch cầu ái toan (EGID). Việc không có tiền sử đi lại, xét nghiệm phân và huyết thanh học âm tính, cùng sự hiện diện của các triệu chứng hệ thống (hen suyễn, viêm xoang, bệnh lý thần kinh) là bằng chứng chống lại nhiễm ký sinh trùng. Việc thiếu các rối loạn tạo máu dòng clonal cùng sự hiện diện của bệnh hen suyễn và các đặc điểm viêm mạch (mặc dù chưa được xác nhận qua mô bệnh học) làm cho khả năng mắc HES thấp hơn. Mặc dù EGID có thể gây ra thâm nhiễm bạch cầu ái toan xuyên thành và gây hẹp, sự kết hợp với các biểu hiện ngoài đường tiêu hóa như bệnh lý thần kinh và tiền sử hen suyễn kéo dài ủng hộ mạnh mẽ chẩn đoán EGPA.
The patient presented with elevated eosinophil levels and symptoms of neurological impairment. Pathological findings from the duodenal bulb revealed significant eosinophilic infiltration. Considering these findings and the patient’s history of asthma, and based on the 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria 3, a diagnosis of EGPA was established.
Bệnh nhân có biểu hiện tăng mức bạch cầu ái toan và các triệu chứng suy giảm thần kinh. Kết quả giải phẫu bệnh từ hành tá tràng cho thấy sự thâm nhiễm bạch cầu ái toan đáng kể. Xem xét các kết quả này cùng với tiền sử hen suyễn của bệnh nhân, và dựa trên Tiêu chuẩn Phân loại của Đại học Thấp khớp Hoa Kỳ/Liên minh Châu Âu về Chống Thấp khớp năm 2022 3, chẩn đoán EGPA đã được xác lập.
Following assessment of the poor prognostic factors using the five-factor score 4, the patient was treated with methylprednisolone tablets (0.8 mg/kg, orally, once daily, reduced dosage after 2 months) and cyclophosphamide (5 mg/kg, IV infusion every 2 weeks, a total of 3 months of treatment) during the induction remission phase. Subsequently, after 3 months, cyclophosphamide was replaced with mycophenolate mofetil (0.5 g, orally, twice daily) during the maintenance remission phase. Considering the patient’s history of hepatitis B and the use of immunosuppressive medications, entecavir (0.5 mg, orally, once daily) was administered for antiviral treatment. In addition, concomitant routine medications included calcium carbonate (0.6 g, orally, once daily) and omeprazole enteric-coated capsules (20 mg, orally, once daily). Prophylaxis against Pneumocystis jirovecii pneumonia with trimethoprim-sulfamethoxazole was also initiated.
Sau khi đánh giá các yếu tố tiên lượng xấu bằng thang điểm 5 yếu tố 4, bệnh nhân được điều trị bằng viên nén methylprednisolone (0.8 mg/kg, uống, một lần mỗi ngày, giảm liều sau 2 tháng) và cyclophosphamide (5 mg/kg, truyền tĩnh mạch mỗi 2 tuần, tổng cộng 3 tháng điều trị) trong giai đoạn cảm ứng lui bệnh. Sau đó, sau 3 tháng, cyclophosphamide được thay thế bằng mycophenolate mofetil (0.5 g, uống, hai lần mỗi ngày) trong giai đoạn duy trì lui bệnh. Xem xét tiền sử viêm gan B của bệnh nhân và việc sử dụng các thuốc ức chế miễn dịch, entecavir (0.5 mg, uống, một lần mỗi ngày) đã được sử dụng để điều trị kháng virus. Ngoài ra, các thuốc thường quy đi kèm bao gồm canxi cacbonat (0.6 g, uống, một lần mỗi ngày) và viên nang bao tan trong ruột omeprazole (20 mg, uống, một lần mỗi ngày). Dự phòng viêm phổi do Pneumocystis jirovecii bằng trimethoprim-sulfamethoxazole cũng đã được bắt đầu.
At the 4-month follow-up, the patient experienced significant alleviation of abdominal distension and pain, with no reported joint pain. In addition, the peripheral blood eosinophil percentage, ESR, and CRP levels in this patient remained within the reference ranges. Follow-up gastroscopy performed at an external hospital in another city revealed marked improvement in duodenal bulb edema and luminal patency, with only mild residual deformity observed.
Tại thời điểm theo dõi 4 tháng, bệnh nhân đã giảm đáng kể tình trạng chướng bụng và đau, không còn đau khớp. Ngoài ra, tỷ lệ bạch cầu ái toan trong máu ngoại vi, ESR và CRP ở bệnh nhân này vẫn nằm trong ngưỡng tham chiếu. Nội soi dạ dày theo dõi tại một bệnh viện bên ngoài ở thành phố khác cho thấy sự cải thiện rõ rệt tình trạng phù nề hành tá tràng và độ thông suốt của lòng ống, chỉ còn quan sát thấy biến dạng tồn dư nhẹ.
Discussion
Bàn luận
EGPA VS EGID
EGPA VÀ EGID
A key diagnostic challenge in this case was distinguishing EGPA from EGID, as both can cause significant eosinophilic infiltration of the gastrointestinal tract, leading to stenosis. EGID is primarily a disorder confined to the gastrointestinal tract, although rare extra-intestinal manifestations can occur. The diagnosis of EGID requires the exclusion of other causes of eosinophilia, including EGPA. Our patient’s well-established history of asthma, the presence of sensorineural hearing loss (suggesting extra-intestinal organ involvement), and sinusitis are features that are not typical of EGID and are core components of the EGPA classification criteria. Therefore, despite the absence of vasculitis on the superficial mucosal biopsy, the constellation of systemic findings firmly supports EGPA as the unifying diagnosis.
Một thách thức chẩn đoán quan trọng trong ca bệnh này là việc phân biệt EGPA với EGID, vì cả hai đều có thể gây ra sự thâm nhiễm bạch cầu ái toan đáng kể ở đường tiêu hóa, dẫn đến hẹp. EGID chủ yếu là một rối loạn khu trú ở đường tiêu hóa, mặc dù các biểu hiện ngoài đường tiêu hóa hiếm gặp vẫn có thể xảy ra. Chẩn đoán EGID đòi hỏi phải loại trừ các nguyên nhân khác gây tăng bạch cầu ái toan, bao gồm cả EGPA. Tiền sử hen suyễn đã được xác định rõ ràng của bệnh nhân, sự hiện diện của tình trạng mất thính lực tiếp nhận (gợi ý tổn thương cơ quan ngoài đường tiêu hóa) và viêm xoang là những đặc điểm không điển hình của EGID và là các thành phần cốt lõi trong tiêu chuẩn phân loại EGPA. Do đó, bất chấp việc không tìm thấy viêm mạch trên sinh thiết niêm mạc bề mặt, tập hợp các phát hiện hệ thống củng cố vững chắc chẩn đoán EGPA là chẩn đoán xác định.
Moreover, there have been limited reports of EGPA cases involving the gastrointestinal system. Yagi et al reported the first case of EGPA-like vasculitis in a child presenting with acute pancreatitis, revealing marked eosinophil infiltration in the pancreas upon autopsy 7. Ye et al reported multiple cases of cholecystitis complicated with EGPA through pathological examination of resected gallbladders. Among these patients, 91.7% exhibited favorable responses to steroid and immunosuppressant therapies 8. In patients with eosinophilic gastrointestinal diseases, eosinophilic infiltration of the muscular layer of the intestine can lead to local tissue edema and fibrosis, ultimately resulting in intestinal stenosis and obstruction 9. Gastroscopy revealed local edema and stenosis in the duodenal bulb of our patient. These findings suggest a strong association with extensive eosinophil infiltration. The clinical and endoscopic response to immunosuppressive therapy further supports an inflammatory, EGPA-related etiology.
Hơn nữa, các báo cáo về các trường hợp EGPA liên quan đến hệ tiêu hóa còn hạn chế. Yagi và cộng sự đã báo cáo ca bệnh đầu tiên về viêm mạch giống EGPA ở một trẻ em có biểu hiện viêm tụy cấp, cho thấy sự thâm nhiễm bạch cầu ái toan rõ rệt trong tuyến tụy khi khám nghiệm tử thi 7. Ye và cộng sự đã báo cáo nhiều trường hợp viêm túi mật biến chứng cùng EGPA thông qua kiểm tra bệnh lý các túi mật đã phẫu thuật cắt bỏ. Trong số các bệnh nhân này, 91.7% có phản ứng thuận lợi với liệu pháp steroid và thuốc ức chế miễn dịch 8. Ở những bệnh nhân mắc bệnh tiêu hóa tăng bạch cầu ái toan, sự thâm nhiễm bạch cầu ái toan ở lớp cơ của ruột có thể dẫn đến phù nề và xơ hóa mô tại chỗ, cuối cùng dẫn đến hẹp và tắc nghẽn ruột 9. Nội soi dạ dày cho thấy phù nề và hẹp cục bộ ở hành tá tràng của bệnh nhân chúng tôi. Những phát hiện này cho thấy mối liên quan chặt chẽ với tình trạng thâm nhiễm bạch cầu ái toan lan rộng. Phản ứng lâm sàng và nội soi đối với liệu pháp ức chế miễn dịch càng củng cố thêm nguyên nhân gây bệnh liên quan đến viêm do EGPA.
The treatment of EGPA remains somewhat controversial, mainly depending on factors such as disease severity, organ involvement, and disease activity. The conventional treatment regimen for EGPA relies on systemic corticosteroids combined with immunosuppressants for severe or refractory diseases. Recent research has highlighted the potential role of inerleukin (IL)-5, a critical factor in eosinophil activation, in the pathogenesis of EGPA. IL-5 not only induces the differentiation and maturation of eosinophils but also inhibits their apoptosis 10. Mepolizumab, the first drug developed and approved for the treatment of severe eosinophilic asthma, functions by inhibiting IL-5-related signal transduction in eosinophils, thereby impeding their activation and tissue accumulation. Recent international guidelines, including the 2024 EULAR updates, reinforce this approach for severe cases 11. A double-blind, randomized, placebo-controlled trial conducted in 2017 demonstrated that mepolizumab notably extended the duration of remission in patients with EGPA, with a higher proportion of individuals achieving remission. Additionally, mepolizumab facilitates a reduction in glucocorticoid dosage 12. Another study showed that the reduction in the use of oral corticosteroids was greater in the mepolizumab-treated group, compared with the placebo group. Moreover, regardless of whether patients with EGPA have previously used immunosuppressants, or the length of the EGPA disease course, mepolizumab can provide clinical benefits 13. In the present case, a combination of corticosteroids and cyclophosphamide was administered for the treatment of EGPA complicated by duodenal stenosis, resulting in a favorable therapeutic outcome. The patient’s symptoms of abdominal distension and pain were significantly alleviated, and disease activity was effectively controlled.
Việc điều trị EGPA vẫn còn một số tranh cãi, chủ yếu phụ thuộc vào các yếu tố như mức độ nghiêm trọng của bệnh, tổn thương cơ quan và hoạt động của bệnh. Phác đồ điều trị thông thường cho EGPA dựa trên việc sử dụng corticosteroid toàn thân kết hợp với thuốc ức chế miễn dịch cho các bệnh nặng hoặc kháng trị. Các nghiên cứu gần đây đã làm nổi bật vai trò tiềm năng của interleukin (IL)-5, một yếu tố quan trọng trong quá trình hoạt hóa bạch cầu ái toan, trong cơ chế bệnh sinh của EGPA. IL-5 không chỉ thúc đẩy quá trình biệt hóa và trưởng thành của bạch cầu ái toan mà còn ức chế quá trình chết theo chương trình (apoptosis) của chúng 10. Mepolizumab, loại thuốc đầu tiên được phát triển và phê duyệt để điều trị hen suyễn tăng bạch cầu ái toan nghiêm trọng, hoạt động bằng cách ức chế quá trình truyền tín hiệu liên quan đến IL-5 trong bạch cầu ái toan, từ đó cản trở sự hoạt hóa và tích tụ tại mô. Các hướng dẫn quốc tế gần đây, bao gồm các bản cập nhật EULAR năm 2024, củng cố phương pháp này cho các trường hợp nghiêm trọng 11. Một thử nghiệm mù đôi, ngẫu nhiên, có đối chứng với giả dược thực hiện năm 2017 đã chứng minh rằng mepolizumab làm kéo dài đáng kể thời gian lui bệnh ở bệnh nhân EGPA, với tỷ lệ cá nhân đạt được sự lui bệnh cao hơn. Ngoài ra, mepolizumab còn tạo điều kiện giảm liều glucocorticoid 12. Một nghiên cứu khác cho thấy mức độ giảm sử dụng corticosteroid đường uống lớn hơn ở nhóm được điều trị bằng mepolizumab so với nhóm giả dược. Hơn nữa, bất kể bệnh nhân EGPA trước đó đã sử dụng thuốc ức chế miễn dịch hay chưa, hoặc thời gian mắc bệnh EGPA kéo dài bao lâu, mepolizumab đều có thể mang lại những lợi ích lâm sàng 13. Trong trường hợp này, sự kết hợp giữa corticosteroid và cyclophosphamide đã được sử dụng để điều trị EGPA biến chứng hẹp tá tràng, dẫn đến kết quả điều trị thuận lợi. Các triệu chứng chướng bụng và đau của bệnh nhân đã giảm đáng kể, và hoạt động của bệnh được kiểm soát hiệu quả.
Conclusions
Kết luận
This case of ANCA-negative EGPA presenting with duodenal stenosis highlights a rare but significant gastrointestinal manifestation of the disease, likely driven by intense eosinophilic infiltration leading to tissue edema and fibrotic stenosis. While the superficial biopsies did not demonstrate vasculitis, the diagnosis was confirmed by fulfilling recognized classification criteria based on clinical features. We hypothesize that in ANCA-negative EGPA, dense eosinophilic infiltration may preferentially affect the gastrointestinal muscular layer, leading to obstructive complications; however, this observation from a single case requires validation in larger cohorts, as the generalizability of these observations is limited by the nature of a single case report. We recommend that EGPA be considered in the differential diagnosis for patients with a history of asthma or chronic respiratory disease who present with eosinophilia and unexplained gastrointestinal symptoms, such as obstruction, pancreatitis, or cholecystitis. Further cohort studies are needed to validate these recommendations.
Ca bệnh EGPA âm tính với ANCA biểu hiện bằng hẹp tá tràng này làm nổi bật một biểu hiện tiêu hóa hiếm gặp nhưng quan trọng của bệnh, có khả năng do tình trạng thâm nhiễm bạch cầu ái toan dữ dội dẫn đến phù nề mô và hẹp xơ hóa. Mặc dù các mẫu sinh thiết bề mặt không cho thấy viêm mạch, chẩn đoán đã được xác nhận bằng cách đáp ứng các tiêu chuẩn phân loại được công nhận dựa trên các đặc điểm lâm sàng. Chúng tôi giả thuyết rằng trong EGPA âm tính với ANCA, sự thâm nhiễm bạch cầu ái toan dày đặc có thể ưu tiên ảnh hưởng đến lớp cơ đường tiêu hóa, dẫn đến các biến chứng tắc nghẽn; tuy nhiên, quan sát từ một ca bệnh đơn lẻ này cần được xác nhận trong các nhóm đối tượng lớn hơn, vì tính khái quát hóa của những quan sát này bị hạn chế bởi bản chất của một báo cáo ca bệnh. Chúng tôi khuyến nghị rằng nên cân nhắc EGPA trong chẩn đoán phân biệt đối với những bệnh nhân có tiền sử hen suyễn hoặc bệnh hô hấp mãn tính xuất hiện tình trạng tăng bạch cầu ái toan và các triệu chứng tiêu hóa không rõ nguyên nhân, chẳng hạn như tắc nghẽn, viêm tụy hoặc viêm túi mật. Các nghiên cứu theo nhóm (cohort) sâu hơn là cần thiết để xác nhận những khuyến nghị này.
Reference
- Cottin V, Bel E, Bottero Pthe Groupe d’Etudes et de Recherche sur les Maladies Orphelines Pulmonaires (GERM“O”P), Respiratory manifestations of eosinophilic granulomatosis with polyangiitis (Churg-Strauss): Eur Respir J, 2016; 48(5); 1429-41
- Comarmond C, Pagnoux C, Khellaf MFrench Vasculitis Study Group, Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): Clinical characteristics and long-term followup of the 383 patients enrolled in the French Vasculitis Study Group cohort: Arthritis Rheum, 2013; 65(1); 270-81
- Grayson PC, Ponte C, Suppiah RDCVAS Study Group, 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis: Ann Rheum Dis, 2022; 81(3); 309-14
- Nguyen Y, Guillevin L, Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): Semin Respir Crit Care Med, 2018; 39(4); 471-81
- Trivioli G, Terrier B, Vaglio A, Eosinophilic granulomatosis with polyangiitis: Understanding the disease and its management: Rheumatology (Oxford), 2020; 59(Suppl 3); iii84-iii94
- Nishi R, Koike H, Ohyama K, Differential clinicopathologic features of EGPA-associated neuropathy with and without ANCA: Neurology, 2020; 94(16); e1726-e37
- Yagi H, Takahashi S, Kibe T, An autopsy case of a 5-year-old child with acute pancreatitis caused by eosinophilic granulomatosis with polyangiitis-like necrotizing vasculitis: Case Rep Rheumatol, 2019; 2019; 9053747
- Ye L, Lu X, Xue J, Eosinophilic granulomatosis with polyangiitis complicated by cholecystitis: a case report and review of the literature: Clin Rheumatol, 2016; 35(1); 259-63
- Yun MY, Cho YU, Park IS, Eosinophilic gastroenteritis presenting as small bowel obstruction: A case report and review of the literature: World J Gastroenterol, 2007; 13(11); 1758-60
- Furuta S, Iwamoto T, Nakajima H, Update on eosinophilic granulomatosis with polyangiitis: Allergol Int, 2019; 68(4); 430-36
- Hellmich B, Sanchez-Alamo B, Schirmer JH, EULAR recommendations for the management of ANCA-associated vasculitis: 2022 update: Ann Rheum Dis, 2024; 83(1); 30-47
- Wechsler ME, Akuthota P, Jayne DEGPA Mepolizumab Study Team, Mepolizumab or placebo for eosinophilic granulomatosis with polyangiitis: N Engl J Med, 2017; 376(20); 1921-32
- Jayne DRW, Terrier B, Hellmich B, Mepolizumab has clinical benefits including oral corticosteroid sparing irrespective of baseline EGPA characteristics: ERJ Open Res, 2024; 10(1); 00509-2023
Có thể bạn quan tâm
-
Nhiễm trùng vắc-xin Bacillus Calmette-Guérin lan tỏa tiến triển nhanh (Viêm hạch BCG) ở trẻ sơ sinh 3 tháng tuổi không có suy giảm miễn dịch: Báo cáo ca bệnh
Rapidly Progressive Disseminated Bacillus Calmette-Guérin Infection (BCGitis) in a 3-Month-Old Infant Without Immunodeficiency: A Case Report
-
Liệu pháp miễn dịch kết hợp hóa trị so với hóa trị đơn thuần trong điều trị ung thư vú thể tam âm giai đoạn sớm
Immunotherapy plus chemotherapy versus chemotherapy alone for early triple-negative breast cancer
-
Bạn có đang tập thể dục vào sai thời điểm không? Đồng hồ sinh học của bạn có thể ảnh hưởng đến việc tập luyện của bạn như thế nào
Are you exercising at the wrong time? How your body clock can affect your workouts