Ca lâm sàng
U nhầy ruột thừa độ ác tính thấp phát hiện tình cờ trong ca mổ lấy thai: Báo cáo ca lâm sàng
Low-Grade Appendiceal Mucinous Neoplasm as an Incidental Finding During Cesarean Section: A Case Report
Vesna Paunovic; Tomislav Paunovic; Aleksa Jokic; Bojana S. Ivic; Aleksandra Petrovic; Nina Pejic; Milos Stulic; Jelena Martinov Nestorov; Jovan Jevtic; Zeljko Vlaisavljevic. American Journal of Case Reports. doi: 10.12659/AJCR.949554. Open access.
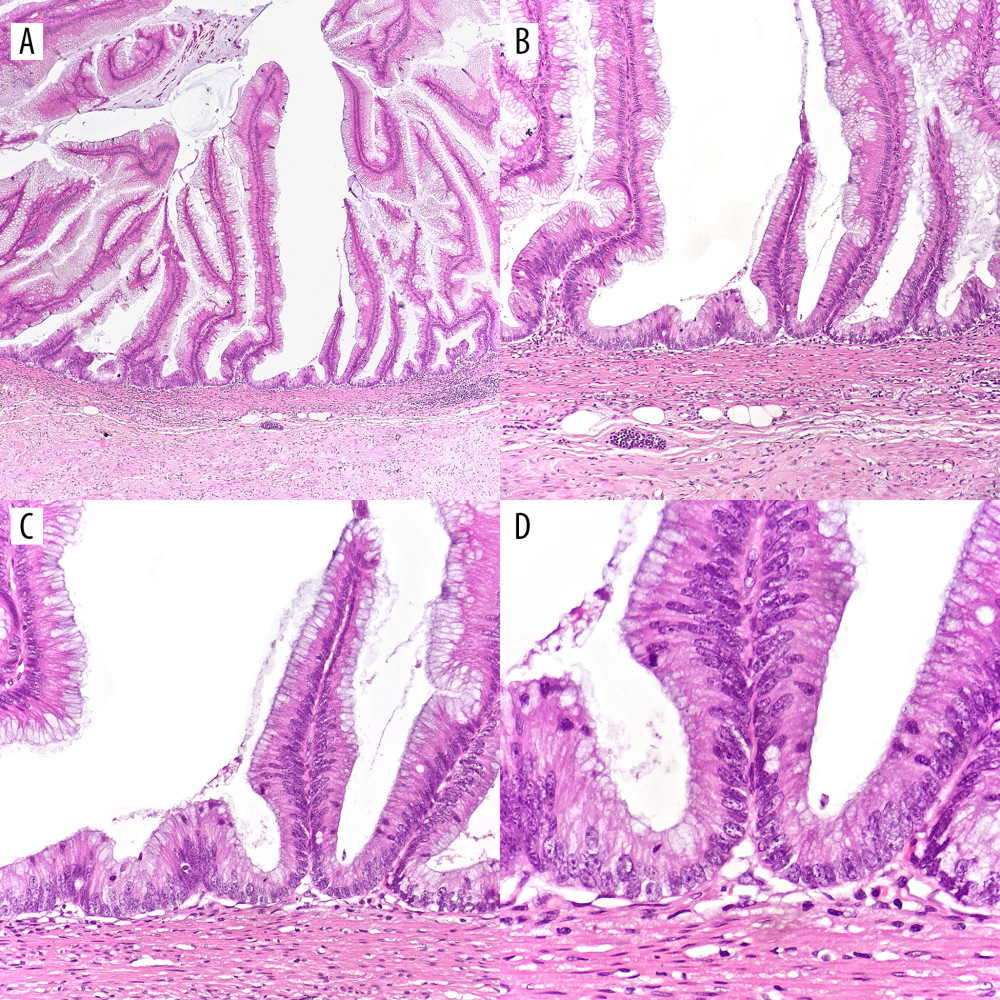
Figure 1
https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e949554-g001.jpg&idArt=949554&w=1000
Figure 1
Hình 1
(A–D) Low-grade appendiceal mucinous neoplasm (LAMN). (A–C) Proliferation of mucinous epithelial cells forming villous structures within the appendiceal lumen. The underlying lymphoid tissue is atrophic, and the muscularis mucosae is effaced. Subepithelial fibrosis is present, and the lesion demonstrates a pushing (non-infiltrative) growth pattern. (D) The lesional epithelium shows abundant apical mucin and elongated nuclei with mild (low-grade) cytologic atypia. (H&E; magnifications: A ×40; B ×100; C ×200; D ×400).
(A–D) U nhầy ruột thừa độ ác tính thấp (LAMN). (A–C) Sự tăng sinh của các tế bào biểu mô nhầy tạo thành các cấu trúc nhung mao bên trong lòng ruột thừa. Mô bạch huyết bên dưới bị teo và lớp cơ niêm bị xóa mờ. Có tình trạng xơ hóa dưới biểu mô và tổn thương thể hiện kiểu phát triển đẩy lồi (không xâm lấn). (D) Biểu mô tổn thương cho thấy lượng chất nhầy dồi dào ở đỉnh và nhân kéo dài với dị dạng tế bào mức độ nhẹ (độ ác tính thấp). (H&E; độ phóng đại: A ×40; B ×100; C ×200; D ×400).
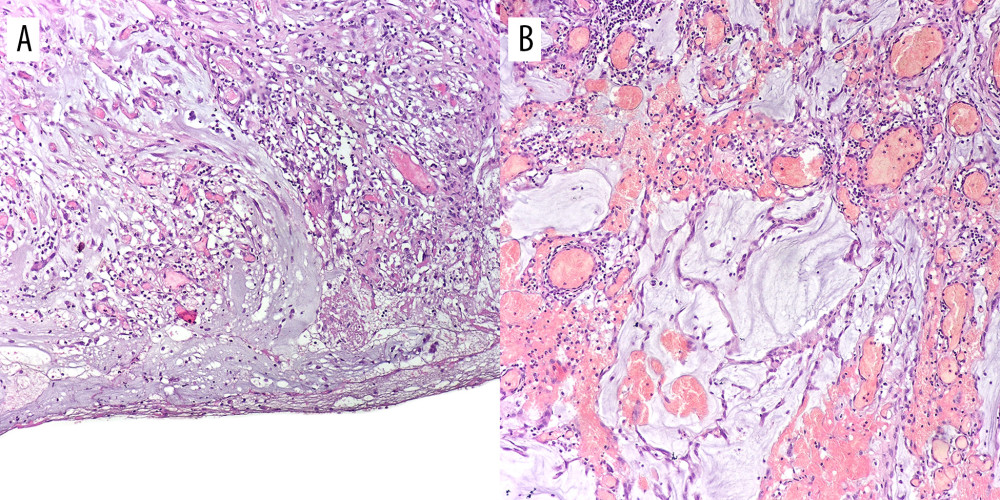
Figure 2
https://jours.isi-science.com/imageXml.php?i=amjcaserep-26-e949554-g002.jpg&idArt=949554&w=1000
Figure 2
Hình 2
(A, B) Extruded mucin. (A) Mucin pools covering the serosa with a prominent granulation tissue response. (B) Extruded mucin surrounded by granulation tissue composed of fibroblasts, blood vessels and inflammatory cells. (H&E; magnifications: ×100).
(A, B) Chất nhầy thoát vị. (A) Các bể chất nhầy bao phủ lớp thanh mạc với phản ứng mô hạt nổi bật. (B) Chất nhầy thoát vị được bao quanh bởi mô hạt cấu thành từ các nguyên bào sợi, mạch máu và các tế bào viêm. (H&E; độ phóng đại: ×100).
Có thể bạn quan tâm
-
Đáp ứng với hormone tăng trưởng ở trẻ có đột biến TOMM7 đồng hợp tử: Những góc nhìn điều trị mới
Growth Hormone Response in a Child With a Homozygous TOMM7 Mutation: Novel Therapeutic Insights
-
Hiệu quả của điều trị bằng thuốc so với giả dược hoặc không điều trị trong kiểm soát tình trạng mệt mỏi sau chấn thương sọ não (TBI)
Effects of pharmacological treatment compared with placebo or no treatment for fatigue management after traumatic brain injury (TBI)
-
Điều trị bằng kháng sinh cho bệnh đau lưng dưới, đau rễ thần kinh, hoặc cả hai
Antibiotic treatment for low back pain, radicular pain, or both
-
Thanh thiếu niên chuyển giới và gia đình họ gặp khó khăn trong việc tìm kiếm dịch vụ chăm sóc xác nhận giới tính – ngay cả ở những tiểu bang mà dịch vụ này vẫn hợp pháp.
Transgender youth and their families struggle to find gender-affirming care – even in states where it’s still legal